Definition
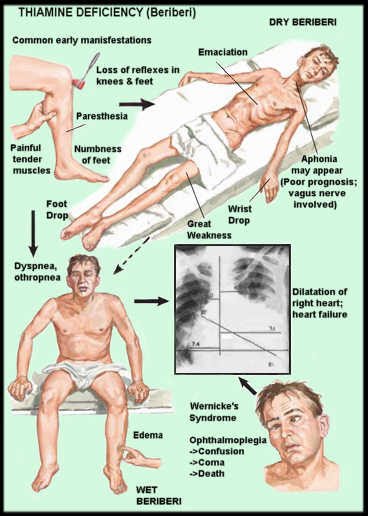
Wernicke’s encephalopathy is a serious neurological condition that results primarily from a deficiency of the nutrient thiamine which is also known as Vitamin B1. This condition is an inflammatory, hemorrhagic, degenerative condition of the brain. It is characterized by lesions in several parts of the brain, including the hypothalamus, mammillary bodies, and tissues surrounding the ventricles and aqueducts, double vision, ophthalmoplegia, involuntary and rapid movements of the eyes, lack of muscular coordination, and decreased mental function, which may be mild or severe. The disease is comprised of three main symptoms: mental confusion, lack of muscle coordination, and a paralysis of the muscles which control eye movements.
Frequency
- The male-to-female ratio is 1.7:1, likely owing to alcoholism being 3-4 times more frequent in men than in women.
- Wernicke encephalopathy have placed the incidence between 0.8% and 2.8% of the general population
- The incidence can be as high as 12.5% in a population of alcoholics
Causes
- This disease is caused by a lack of thiamin (vitamin B1), which leads to problems with the normal functioning of the brain.
- Thiamine deficiency is characteristically associated with chronic alcoholism, because it affects thiamine uptake and utilization. Most cases of Wernicke’s encephalopathy are rooted in chronic alcohol abuse. Alcohol can, over time, severely impair the body’s ability to absorb thiamine, gradually leading to a deficiency of this nutrient. When someone who is known to abuse alcohol has symptoms such as confusion and gait ataxia, meaning lack of coordination in walking, Wernicke’s encephalopathy should be considered as a possible cause.
- Wernicke encephalopathy may develop in nonalcoholic conditions such as:
- prolonged starvation
- hyperemesis gravidarum (continuous nausea and vomiting during pregnancy)
- bariatric surgery and other gastric bypass surgeries
- HIV-AIDS
- healthy infants given the wrong formulas
- malnutrition
- complication of GI tract disease
- Cancers that have spread throughout the body
- Heart failure (when treated with long-term diuretic therapy)
- Long periods of intravenous (IV) therapy without receiving thiamine supplements
- Long-term dialysis
- Very high thyroid hormone levels (thyrotoxicosis)
- Chronic renal failure
- Carbohydrate loading in the presence of marginal thiamine stores (feeding after starvation)
- Absence of thiamine from the diet (in the case of infants fed formula without the addition of thiamine)
- Congenital transketolase function abnormalities
Signs and Symptoms
TRIAD SYMPTOMS
The 3 components of the classic triad of Wernicke encephalopathy are encephalopathy, ataxic gait, and some variant of oculomotor dysfunction.
- Encephalopathy. Encephalopathy is characterized by a global confusional state, disinterest, inattentiveness, or agitation. The most constant symptoms of Wernicke encephalopathy are the mental status changes. Stupor and coma are rare.
- Loss of muscular coordination (ataxia) – Leg tremor. Gait ataxia is often a presenting symptom. Ataxia is likely to be a combination of polyneuropathy, cerebellar damage, and vestibular paresis. Vestibular dysfunction, usually without hearing loss, is universally impaired in the acute stages of Wernicke encephalopathy.
- Ocular Abnormalities. Ocular abnormalities are the hallmarks of Wernicke encephalopathy. The oculomotor signs are:
- Abnormal eye movement (back and forth movements called nystagmus) – most common
- Double vision
- Eyelid drooping
- bilateral lateral rectus palsies
- conjugate gaze palsies reflecting cranial nerve involvement of the oculomotor, abducens, and vestibular nuclei
- pupillary abnormalities such as sluggishly reactive pupils, ptosis, scotomata, and anisocoria
OTHER SYMPTOMS
- Vestibular dysfunction
- Hypotension. Hypotension can be secondary to thiamine deficiency either through cardiovascular beriberi or thiamine deficiency–induced autonomic dysfunction.
- Hypothermia. Thiamine deficiency often affects the temperature-regulating center in the brainstem, which can result in hypothermia.
- Coma
- Wet beriberi
- Nutritional polyneuropathy
- Muscle atrophy,
- Cold skin.
- Loss of memory, can be profound.
- Swallowing difficulties,
- Double vision.
- Abnormal eye movements.
- Inability to form new memories.
- Dry skin,
- Staggering gait.
- Eye movement abnormalities.
- Difficulty with speech,
- Confabulation (making up stories).
- Reduced eye movement.
Diagnosis
No specific laboratory test is available for diagnosing Wernicke encephalopathy. Wernicke encephalopathy is a clinical diagnosis, and normal electrolyte levels may only give false reassurance and delay therapy. This is particularly the case where malnutrition is likely to be present. The motto should be “If in doubt, treat,” as administration of thiamine does not pose potential harm.
A Diagnosis can be made by treating the patient with thiamin and watching the symptoms improve. There are blood and urine tests available to check the level of thiamin, but giving the patient thiamin and seeing the response is the best way to diagnose this condition.
- When a person appears poorly nourished (malnourish). The following should be done to check the patient’s nutrition level:
- Serum albumin. This test relates to the person’s general nutrition
- Serum vitamin B1 levels
- Transketolase activity in the red blood cells. The level of this is reduced in people with thiamine deficiency.
- Blood pyruvate and lactate measurements. These tests are sensitive and helpful, as thiamine is a cofactor of the pyruvate dehydrogenase enzyme, an important enzyme in aerobic metabolism.
- Toxic drug screening is performed to exclude some causes of drug-induced altered mental status.
- To exclude hypoglycemia and hyperglycemia, serum glucose levels should be obtained.
- Complete blood cell (CBC) count rules out severe anemias and leukemias as causes of altered mental status.
Treatment
- Intravenous thiamine is given to the patient for a few days until it can be given by mouth.
- The most effective treatment is to eat properly.
- Start thiamine prior to or concurrently with treatment of intravenous glucose solutions, and continue until the patient resumes a normal diet.
- Patients with Wernicke encephalopathy are likely hypomagnesemic and should be treated empirically with parenteral magnesium sulfate, as they may be unresponsive to parenteral thiamine in the presence of hypomagnesemia. After correction of hypomagnesemia in conjunction with thiamine repletion, the blood transketolase activity can return to normal and clearing of the clinical signs may occur.
- Stabilize airway, ensure oxygenation and maintain the patient’s blood pressure as patients with Wernicke’s encephalopathy present with an altered mental status in prehospital settings.
- Promoting hydration.
- Providing proper nutrition.
