Description
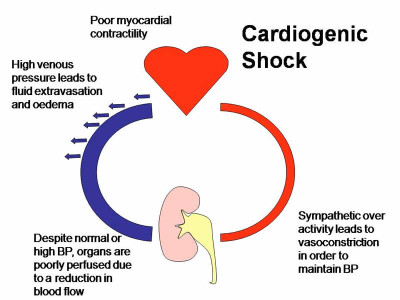
Cardiogenic shock is the inability to meet the metabolic needs due to severely impaired contractility of either ventricle. That leads to decreased tissue perfusion and a shock like state. Risk factor includes prior myocardial infarction, advanced age, female, diabetes, or anterior wall myocardial infarction. The most common cause of cardiogenic shock are acute Myocardial infarction, ventricular septal defect, acute mitral regurgitation, cardiac tamponade, aortic dissection, massive pulmonary infarct, and severe dysrhythmias.
Signs and Symptoms
- Pale, cool and clammy skin
- Pulmonary congestion and hypoxemia worsen as the ventricles fail to eject adequate volume and the blood backs up into the lung.
- Tissue hypoperfusion continues because the oxygen does not meet the metabolic needs.
Physical Examination
Appearance
- Restlessness progressing to unresponsiveness
- Chest pain
- Dysrhythmias
Vital signs
- HR: >100 beats/min
- BP: <80 mm Hg
- RR: > 20 breaths/min
Neurologic
- Agitation
- Restlessness progressing to unresponsiveness, and changes in level of consciousness.
Cardiovascular
- Weak thready pulses
- Rhythm may be irregular
Pulmonary
- Orthopnea
- Crackles
- Cough with increased secretions.
Acute Care Patient Management
Nursing Diagnosis: Impaired gas exchange related to increased left ventricular diastolic pressure (LVEDP) and pulmonary edema associated with severe left ventricular (LV) dysfunction.
Outcome Criteria
- Patient alert and oriented
- Pao2 80 to 100 mm Hg
- pH 7.35 to 7.45
- Paco2 35 to 45 mm Hg
- O2 sat ?95 %
- RR 12 to 20 breaths/min, eupnea
- Lungs clear to auscultation
Nursing Interventions
Patient Monitoring
- Continuously monitor oxygenation status with pulse oximetry.
- Monitor for desaturation in response to nursing intervention.
- Monitor ECG for dysrhythmias caused by hypoxemia, electrolyte imbalances, or ventricular dysfunction.
- Monitor fluid volume status.
Patient Assessment
- Obtain HR, RR, and BP every 15 minutes to evaluate the patient’s response to therapy and detect cardiopulmonary deterioration.
- Assess the patient’s respiratory status. The use of accessory muscles and inability to speak suggest worsening pulmonary congestion.
- Assess for excess fluid volume, which can further compromise myocardial function.
Diagnostic Assessment
- Review ABGs for decreasing trend in Pao2 (hypoxemia) or pH (acidosis). These conditions can adversely affect myocardial contractility.
- Review serial chest radiographs to evaluate the patient’s progress or a worsening lung condition.
Patient Management
- Provide supplemental oxygen as ordered. If the patient develops respiratory distress, be prepared for intubation and mechanical ventilation.
- Administer low-dose morphine sulfate as ordered to reduce preload in an attempt to decrease pulmonary congestion.
- Minimize oxygen demand by maintaining bed rest and decreasing anxiety, fever, and pain.
- Position the patient for maximum chest excursion and comfort.
- Administer diuretics and /or vasodilators as ordered to reduce circulating volume and decrease preload.
 Nursing Management")
