Notes
Description
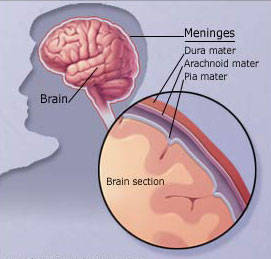
- Meningitis is inflammation of the arachnoid and pia mater of the brain and spinal cord.
- Meningitis is caused by bacterial and viral organisms, although fungal and protozoal meningitis also occurs.
- Cerebrospinal fluid is analyzed to determine the diagnosis and the type of meningitis.
Transmission
- Transmission is by direct contact, including droplet spread.
- Transmission occurs in areas of high population density, crowded living areas, and prisons.
Causes
- Meningitis is most frequently caused by bacterial or viral agents.
- In newborns, Streptococcus pneumoniae is the most frequent bacterial organism; in other age groups, it is S. pneumonia and Neisseria meningitidis. Haemophilus influenzae is the most common organism in unvaccinated children and adults who contract meningitis.
- Viral meningitis is caused by many viruses. Depending on the cause, isolation precautions may be indicated early in treatment. There has been a decrease in viral meningitis in locations where immunizations have become routine.
Predisposing Factors
- Skull fractures
- Brain or spinal surgery
- Sinus or upper respiratory infections
- Use of nasal sprays
- Individuals with a compromised immune system
Assessment
- Mild lethargy
- Memory changes
- Short attention span
- Personality and behavior changes
- Severe headache
- Generalized muscle aches and [pains
- Nausea and vomiting
- Fever and chills
- Tachycardia
- Deterioration in the level of consciousness
- Photophobia
- Signs of meningeal irritation such as nuchial rigidity and positive Kernig’s sign and Brudzinski’s sign
- Red, macular rash with meningococcal meningitis
- Abdominal and chest pain with viral meningitis
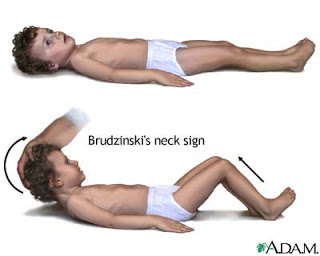
Brudzinski’s sign. Severe neck stiffness causes a patient’s hips and knees to flex when the neck is flexed.

Kernig’s sign. Severe stiffness of the hamstrings causes an inability to straighten the leg when the hip is flexed to 90 degrees.
Possible Complications
- Brain damage
- Hearing loss or deafness
- Hydrocephalus
- Loss of vision
Primary Nursing Diagnosis
- Infection related to pathogens in the CSF
Diagnostic Evaluation
- Lumbar puncture for cerebrospinal fluid (CSF) analysis reveals positive cultures with invading microorganism; sensitivities identify antibiotics that will kill bacteria; cells: 200/μL; protein: elevated >50 mg/dL (viral) and >500 mg/dL (bacterial); glucose: <45 mg/dL; color: may be cloudy or hazy; pressure: elevated; gram stain: bacteria stain either gram positive (blue) or gram negative (red). Lumbar puncture for cerebrospinal fluid (CSF) analysis identifies invading microorganisms. Increased protein occurs as the result of the presence of viruses or bacteria; glucose is decreased as microorganisms use glucose for metabolism. Lumbar puncture is not done in the presence of known increased intracranial pressure.
- Other Tests: Brain scan, computed tomography (CT) scan, magnetic resonance imaging (MRI), cultures and sensitivities (blood, nasal swab, urine), C-reactive protein, complete blood count, counter -immunoelectrophoresis (to determine presence of viruses or protozoa in CSF), chest x-ray
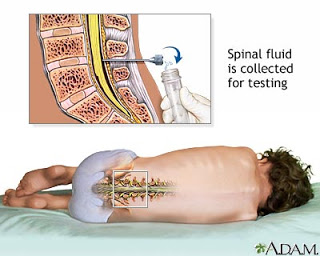
A lumbar puncture, or spinal tap, is a procedure to collect cerebrospinal fluid to check for the presence of disease or injury. A spinal needle is inserted, usually between the 3rd and 4th lumbar vertebrae in the lower spine. Once the needle is properly positioned in the subarachnoid space (the space between the spinal cord and its covering, the meninges), pressures can be measured and fluid can be collected for testing.
Medical Management
- The most critical treatment is the rapid initiation of antibiotic therapy. In addition, assessment and maintenance of airway, breathing, and circulation (ABCs) are essential. Treatment with intubation, mechanical ventilation, and hyperventilation may occur if the patient’s airway and breathing are threatened. Serial neurological assessments and vital signs not only monitor critical changes in the patient but also monitor the patient’s response to therapy. Supportive measures such as bedrest and temperature control with antipyretics or hypothermia limit oxygen consumption. Gradual treatment of hyperthermia is required to prevent shivering.
- Other strategies to manage increased ICP include osmotic diuretics, such as mannitol, or intraventricular CSF drainage and ICP pressure monitoring. Fluids are often restricted if signs of cerebral edema or excessive secretion of antidiuretic hormone are present. If the patient experiences seizures, the physician prescribes anticonvulsant medications. Surgical interventions or CSF drainage may be required to prevent permanent neurological deficits as a result of complications such as hydrocephalus or abscesses. The patient is likely to have a severe headache from increased ICP. Because large doses of narcotic analgesia mask important neurological changes, most physicians prescribe a mild analgesic to decrease discomfort. In children, pain relief decreases crying and fretting, which if left untreated, have the potential to aggravate increased ICP.
- Rehabilitation begins with the acute phase of the illness but becomes increasingly important as the infection subsides. If residual neurological dysfunction is present as a result of irritation, pressure, or brain and nerve damage, an individualized rehabilitation program with a multidisciplinary team is required. Vision and auditory testing should be done at discharge and at intervals during long-term recovery because early interventions for these deficits are needed to prevent developmental delays.
Pharmacologic Highlights
- Antimicrobial therapy: penicillin (or piperacillin or ampicillin), or one of the cephalosporins. The treatment for cryptococcal meningitis is intravenous administration of amphotericin B; may be used with or without 5-flucytosine.
- Vancomycin hydrochloride, alone or in combination with rifampin, may be used if resistant strains of bacteria are identified.
- Dexamethasone may be beneficial as adjunct therapy for acute bacterial meningitis and pneumococcal meningitis.
- Fluid volume expanders are used to treat dehydration and shock.
- Diazepam (Valium) or phenytoin (Dilantin) is used to control seizures.
- An osmotic diuretic, such as mannitol, is used to treat cerebral edema.
Nursing Interventions
- Monitor vital signs and neurological signs.
- Assess for signs of increasing ICP.
- Initiate seizure precautions.
- Monitor for seizure activity.
- Monitor for signs of meningeal irritation.
- Perform cranial nerve assessment.
- Assess peripheral vascular status.
- Maintain isolation precautions as necessary with bacterial meningitis.
- Maintain urine and stool precautions with viral meningitis.
- Maintain respiratory isolation for the client with pneumococcal meningitis.
- Elevate the head of the bed 30 degrees, and avoid neck flexion and extreme hip flexion.
- Prevent stimulation and restrict visitors.
- Administer analgesics as prescribed.
- Administer antibiotics as prescribed.
Documentation Guidelines
- Physiological response: Neurological examination; vital signs; presence of fever; adequacy of airway, breathing, and circulation
- Fluid and electrolyte balance: Intake and output, body weight, skin turgor, abnormal serum electrolytes
- Complications: Seizure activity, decreased mental status, fever, increased ICP
Discharge and Home Healthcare Guidelines
- Explain all medications and include the mechanism of action, dosage, route, and side effects.
- Explain any drug interactions or food interactions.
- Instruct the patient to notify the primary healthcare provider for signs and symptoms of complications, such as fever, seizures, developmental delays, or behavior changes.
- Provide referrals and teaching specific to the identified neurological deficits.
- Encourage the parents to maintain appropriate activities to facilitate the growth and development of the child.
Exam
Nursing Care Plan
Sample Nursing Care Plan for Meningitis
Nursing Diagnosis
Acute pain
Related to
- infection process
- toxin in the circulation
Nursing Intervention for Meningitis:
- Place the ice bag on his head, cool clothing above the eyes, provide a comfortable head position a little bit high, range of motion exercises and active or passive masage neck muscles.
- Support to find a comfortable position (head rather high-).
- Give range of motion exercises active / passive.
- Use a warm moisturizer, neck or hip.
Nursing Diagnosis
Impaired Physical Mobility
Related to
- neuromuscular damage.
Nursing Intervention for Meningitis:
- Assess the degree of immobilization of the patient.
- Assistive range of motion exercises.
- Give skin care, massage with moisturizer.
- Check the area experiencing tenderness, give air mattresses or water body alignment are functionally notice.
- Provide training programs and the use of mobilization.

