Notes
Definition
One of the most successful surgeries in orthopedics is the total hip replacement. In this procedure, the acetabulum and the head of the femur is replaced with prostheses. In cases where a severely damaged hip is present, an artificial joint is used to replace the non-functional area.
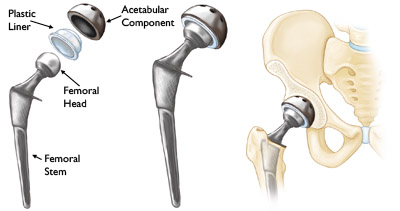
image by: http://orthoinfo.aaos.org/
Indications
Total Hip Replacement surgery is indicated in the following conditions:
- Arthritis such as rheumatoid arthritis and degenerative joint diseases
- Fractures of the femoral neck
- Failure of previous reconstructive surgeries such as failed prostheses, osteotomy and femoral head replacement
- Problems that results from congenital hip disease
Nursing Interventions
It is very important that the nurse is aware that complications might harm the client when left unnoticed and no prompt treatment is carried out on time. Potential complications with this procedure should be made known specifically to the nurse. Nursing care plans should be focused on preventing the occurrence of the following complications:
- Dislocation of the hip prosthesis
- Excessive wound drainage
- Thromboembolism
- Infection
Nursing interventions for possible DISLOCATION OF THE HIP PROSTHESIS
The new hip can be dislocated easily. Thus, the nurse must promote patient teaching on preventing hip prosthesis dislocation which includes the following:
- Patient must be cautioned not to sit too low or cross the legs.
- The patient’s leg should be positioned in ABDUCTION. This is to prevent dislocation of the prosthesis. It is very crucial that the femoral head component of the acetabular cap is maintained in the correct position. Abduction splints, wedge pillows and two or three pillows between the legs of the patient will keep the hip in abduction.
- In cases where the patient needs to be turned, the operative hip must be kept in abduction and the entire length of the leg supported by pillows.
- The hip of the patient should NOT be flexed more than 45 to 60 degrees.
- To prevent acute hip flexion, the head of the bed should not be elevated more than 45 degrees.
- When using the fracture bedpan, the patient is instructed to flex the unoperated hip and use the trapeze to lift the pelvis onto the pan. Instruct the patient not to flex the operated hip.
- Limited flexion is maintained during transfers and when sitting. (see section below on interventions when transferring or sitting the patient who underwent total hip replacement)
- Remind patient not to sleep on the operated side until this position is cleared with the surgeon.
- The nurse should recognize dislocation of the prosthesis which includes:
- Shortening of the leg
- Inability to move the leg
- Malalignment of the leg
- Abnormal rotation
- Increased discomfort
When transferring or sitting the patient who underwent total hip replacement:
- An abduction splint or pillows should be kept between the legs
- The patient is encouraged to keep the operative hip in extension
- The patient is instructed to pivot in the unoperated leg while assisted by the nurse, who protects the operative leg from adduction, flexion and excessive weight-bearing.
- A semi-reclining wheelchair and toilet seat extenders may be used to minimize hip joint flexion.
Nursing Interventions for possible EXCESSIVE WOUND DRAINAGE
- To drain the accumulating blood and fluid at the surgical site, a portable suction device should be used. The accumulation of fluid can contribute to patient discomfort and could provide a site for infection.
- When drainage volumes are greater than expected, the nurse should notify the physician immediately. Expected drainage is 200 to 500 ml in the first 24 hours and by 48 hours postoperatively the total expected drainage in 8 hours usually decreases to 30 ml or less.
- To decrease the homologus blood transfusions, autotransfusion drainage system may be used. This is used when extensive blood loss is anticipated following total hip replacement surgery.
Nursing Interventions for possible Deep Vein Thrombosis
After THR, a thrombus, also known as blood clot, may form in the veins of the client’s thighs, pelvis or leg. Promoting circulation and decreasing the venous stasis are the priorities the nurse must keep in mind after a hip reconstruction.The following are important interventions in preventing thrombus formation:
- Blood thinning agents may be administered to the client as prescribed by the physician. As prophylaxis for DVT following total hip replacement surgery, low-dose heparin or enoxaparin (Lovenax) may be used. Lovenox is a low-molecular weight heparin that requires no routine monitoring of coagulation times.
- Mobilization with ion limits and in proper flexion is encourage.
Nursing Interventions for possible Infection
A small number of people can develop an infection with a total hip replacement. This may require further surgery to remove the prosthetic components and clean out the joint along with a course of antibiotics lasting 6-8 weeks.
- Deep infection may require removal of the implant.
- Identify patients who are at high risk for infection such as those who have diabetes, elderly, obese and poorly nourished.
- Avoid potential sources of infection.
- Administer prophylactic antibiotics.
- Remove indwelling urinary catheters and portable wound suction as soon as possible to prevent infection.
Nursing Care Plans
Nursing Diagnosis
Risk for Infection
Risk factors may include
- Inadequate primary defenses (broken skin, exposure of joint)
- Inadequate secondary defenses/immunosuppression (long-term corticosteroid use, cancer)
- Invasive procedures; surgical manipulation; implantation of foreign body
- Decreased mobility
Possibly evidenced by
- Not applicable. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.
Desired Outcomes
- Achieve timely wound healing, be free of purulent drainage or erythema, and be afebrile.
Nursing Interventions
- Promote good hand washing by staff and patient.
- Rationale: Hand washing is the single most effective way to prevent infection.
- Use strict aseptic or clean techniques as indicated to reinforce or change dressings and when handling drains. Instruct patient not to touch or scratch incision.
- Rationale: Prevents contamination and risk of wound infection, which could require removal of prosthesis.
- Maintain patency of drainage devices (Hemovac, Jackson Pratt) when present. Note characteristics of wound drainage.
- Rationale: Reduces risk of infection by preventing accumulation of blood and secretions in the joint space (medium for bacterial growth). Purulent, nonserous, odorous drainage is indicative of infection, and continuous drainage from incision may reflect developing skin tract, which can potentiate infectious process.
- Assess skin/incision color, temperature, and integrity; note presence of erythema or inflammation, loss of wound approximation.
- Rationale: Provides information about status of healing process and alerts staff to early signs of infection.
- Investigate reports of increased incisional pain, changes in characteristics of pain.
- Rationale: Deep, dull, aching pain in operative area may indicate developing infection in joint. Note: Infection is devastating, because joint cannot be saved once infection sets in, and prosthetic loss will occur.
- Monitor temperature. Note presence of chills.
- Rationale: Although temperature elevations are common in early postoperative phase, elevations occurring 5 or more days postoperatively and/or presence of chills usually requires intervention to prevent more serious complications, e.g., sepsis, osteomyelitis, tissue necrosis, and prosthetic failure.
- Encourage fluid intake, high-protein diet with roughage.
- Rationale: Maintains fluid and nutritional balance to support tissue perfusion and provide nutrients necessary for cellular regeneration and tissue healing.
- Maintain reverse or protective isolation, if appropriate.
- Rationale: May be done initially to reduce contact with sources of possible infection, especially in elderly, immunosuppressed, or diabetic patient.
- Administer antibiotics as indicated.
- Rationale: Used prophylactically in the operating room and first 24 hr to prevent infection.
Nursing Diagnosis
Impaired Physical Mobility
May be related to
- Pain and discomfort, musculoskeletal impairment
- Surgery/restrictive therapies
Possibly evidenced by
- Reluctance to attempt movement, difficulty purposefully moving within the physical environment
- Reports of pain/discomfort on movement
- Limited ROM; decreased muscle strength/control
Desired Outcomes
- Maintain position of function, as evidenced by absence of contracture.
- Display increased strength and function of affected joint and limb. Participate in ADLs/rehabilitation program.
Nursing Interventions
- Maintain affected joint in prescribed position and body in alignment when in bed.
- Rationale: Provides for stabilization of prosthesis and reduces risk of injury during recovery from effects of anesthesia.
- Medicate before procedures and activities.
- Rationale: Muscle relaxants, narcotics, analgesics decrease pain, reduce muscle tension and/or spasm, and facilitate participation in therapy.
- Turn on unoperated side using adequate number of personnel and maintaining operated extremity in prescribed alignment. Support position with pillows and/or wedges.
- Rationale: Prevents dislocation of hip prosthesis and prolonged skin or tissue pressure, reducing risk of tissue ischemia and/or breakdown.
- Demonstrate and assist with transfer techniques and use of mobility aids, e.g., trapeze, walker.
- Rationale: Facilitates self-care and patient’s independence. Proper transfer techniques prevent shearing abrasions of skin and falls.
- Determine upper body strength as appropriate. Involve in exercise program.
- Rationale: Replacement of lower extremity joint requires increased use of upper extremities for transfer activities and use of ambulation devices.
- Inspect skin, observe for reddened areas. Keep linens dry and wrinkle-free. Massage skin and bony prominences routinely. Protect operative heel, elevating whole length of leg with pillow and placing heel on water glove if burning sensation reported.
- Rationale: Prevents skin breakdown and eases irritation.
- Perform and assist with range of motion exercises to unaffected joints.
- Rationale: Patient with degenerative joint disease can quickly lose joint function during periods of restricted activity.
Promote participation in rehabilitative exercise program:
- Total hip: Quadriceps and gluteal muscle setting, isometrics, leg lifts, dorsiflexion, plantar flexion of the foot; Total knee:Quadriceps setting, gluteal contraction, flexion/extension exercises, isometrics;
- Rationale: Strengthens muscle groups, increasing muscle tone and mass; stimulates circulation; prevents decubitus. Active use of the joint may be painful but will not injure the joint. Continuous passive motion (CPM) exercise may be initiated on the knee joint postoperatively.
- Other joints: Exercises are individually designed toes and knee movements; arm and unaffected fingers (for finger-joint replacement), exercise fingers and/or wrist of affected arm (for shoulder replacement).
- Rationale: Meets specific needs of the replaced joint.
- Observe appropriate limitations based on specific joint; avoid marked flexion and/or rotation of hip and flexion or hyperextension of leg; adhere to weight-bearing restrictions; wear knee immobilizer as indicated.
- Rationale: Joint stress is to be avoided at all times during stabilization period to prevent dislocation of new prosthesis.
- Investigate sudden increase in pain and shortening of limb, as well as changes in skin color, temperature, and sensation.
- Rationale: Indicative of slippage of prosthesis, requiring medical evaluation and/or intervention.
- Encourage participation in ADLs.
- Rationale: Enhances self-esteem; promotes sense of control and independence.
- Provide positive reinforcement for efforts.
- Rationale: Promotes a positive attitude and encourages involvement in therapy.
Nursing Diagnosis
Risk for Peripheral Neurovascular Dysfunction
Risk factors may include
- Orthopedic surgery; mechanical compression (e.g., dressing, brace, cast), vascular obstruction, immobilization
Possibly evidenced by
- Not applicable. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.
Desired Outcomes
- Maintain function as evidenced by sensation, movement within normal limits (WNL) for individual situation.
- Demonstrate adequate tissue perfusion as evidenced by palpable pulses, brisk capillary refill, skin warm/dry, and normal color.
Nursing Interventions
- Palpate pulses on both sides. Evaluate capillary refill and skin color and temperature. Compare with non-operated limb.
- Rationale: Diminished or absent pulses, delayed capillary refill time, pallor, blanching, cyanosis, and coldness of skin reflect diminished circulation or perfusion. Comparison with unoperated limb provides clues as to whether neurovascular problem is localized or generalized.
- Assess motion and sensation of operated extremity.
- Rationale: Increasing pain, numbness or tingling, inability to perform expected movements (flex foot) suggest nerve injury, compromised circulation, or dislocation of prosthesis, requiring immediate intervention.
- Test sensation of peroneal nerve by pinch or pinprick in the dorsal web between first and second toe, and assess ability to dorsiflex toes after joint replacement.
- Rationale: Position and length of peroneal nerve increase risk of direct injury or compression by tissue edema or hematoma.
- Monitor vital signs.
- Rationale: Tachycardia and decreasing BP may reflect response to hypovolemia or blood loss or suggest anaphylaxis related to absorption of methyl methacrylate into systemic circulation. Note: This occurs less often because of the advent of prosthetics with a porous layer that fosters ingrowth of bone instead of total reliance on adhesives to internally fix the device.
- Monitor amount and characteristics of drainage on dressings and from suction device. Note swelling in operative area.
- Rationale: May indicate excessive bleeding and hematoma formation, which can potentiate neurovascular compromise. Note: Drainage following hip replacement may reach 1000 cc in early postoperative period, potentially affecting circulating volume.
- Ensure that stabilizing devices (abduction pillow, splint device) are in correct position and are not exerting undue pressure on skin and underlying tissue. Avoid use of pillow or knee gatch under knees.
- Rationale: Reduces risk of pressure on underlying nerves or compromised circulation to extremities.
- Evaluate for calf tenderness, positive Homans’ sign, and inflammation.
- Rationale: Early identification of thrombus development and intervention may prevent embolus formation.
- Observe for signs of continued bleeding, oozing from puncture sites and mucous membranes, or ecchymosis following minimal trauma.
- Rationale: Depression of clotting mechanisms and/or sensitivity to anticoagulants may result in bleeding episodes that can affect red blood cell (RBC) level and circulating volume.
- Observe for restlessness, confusion, sudden chest pain, dyspnea, tachycardia, fever, development of petechiae
- Rationale: Fat emboli can occur (usually in first 72 hr postoperatively) because of surgical trauma and manipulation of bone during implantation of prosthesis.
Monitor laboratory studies:
- Hct
- Rationale: Usually done 24–48 hr postoperatively for evaluation of blood loss, which can be quite large because of high vascularity of surgical site in hip replacement. Note: Monitoring of CBC or repeated count may also be indicated for patients receiving enoxaparin (Lovenox).
- Coagulation studies.
- Rationale: Evaluates presence or degree of alteration in clotting mechanisms and effects of anticoagulant and/or antiplatelet agents when used. Note: Not necessary for patients receiving enoxaparin (Lovenox); however, stool occult blood tests may be indicated.
- Administer medications as indicated: warfarin sodium (Coumadin), heparin, aspirin, low-molecular-weight heparin, e.g., enoxaparin (Lovenox).
- Rationale: Anticoagulants and/or antiplatelet agents may be used to reduce risk of thrombophlebitis and pulmonary emboli.
- Apply cold or heat as indicated.
- Rationale: Ice packs are used initially to limit edema and/or hematoma formation. Heat may then be used to enhance circulation, facilitating resolution of tissue edema.
- Maintain intermittent compression stocking or foot pumps when used.
- Rationale: Promotes venous return and prevents venous stasis, reducing risk of thrombus formation.
- Prepare for surgical procedure as indicated.
- Rationale: Evacuation of hematoma or revision of prosthesis may be required to correct compromised circulation.
Nursing Diagnosis
Acute Pain
May be related to
- Injuring agents: biological, physical/psychological (e.g., muscle spasms, surgical procedure, preexisting chronic joint diseases, elderly age, anxiety)
Possibly evidenced by
- Reports of pain; distraction/guarding behaviors
- Narrowed focus/self-focusing
- Alteration in muscle tone; autonomic responses
Desired Outcomes
- Report pain relieved/controlled.
- Appear relaxed, able to rest/sleep appropriately.
- Demonstrate use of relaxation skills and diversional activities as indicated by individual situation.
Nursing Interventions
- Assess reports of pain, noting intensity (scale of 0–10), duration, and location.
- Rationale: Provides information on which to base and monitor effectiveness of interventions.
- Maintain proper position of operated extremity.
- Rationale: Reduces muscle spasm and undue tension on new prosthesis and surrounding tissues.
- Provide comfort measures (frequent repositioning, back rub) and diversional activities. Encourage stress management techniques (progressive relaxation, guided imagery, visualization, meditation). Provide Therapeutic Touch as appropriate.
- Rationale: Reduces muscle tension, refocuses attention, promotes sense of control, and may enhance coping abilities in the management of discomfort or pain, which can persist for an extended period.
- Medicate on a regular schedule and before activities.
- Rationale: Reduces muscle tension; improves comfort, and facilitates participation.
- Investigate reports of sudden, severe joint pain with muscle spasms and changes in joint mobility; sudden, severe chest pain with dyspnea and restlessness.
- Rationale: Early recognition of developing problems, such as dislocation of prosthesis or pulmonary emboli (blood/fat), provides opportunity for prompt intervention and prevention of more serious complications.
- Administer narcotics, analgesics, and muscle relaxants as needed. Instruct and monitor use of PCA and/or epidural administration.
- Rationale: Relieves surgical pain and reduces muscle tensions and spasm, which contributes to overall discomfort. Narcotic infusion (including epidural) may be given during first 24–48 hr, with oral analgesics added to pain management program as patient progresses. Note: Use of ketorolac (Toradol) or other NSAIDs is contraindicated when patient is receiving enoxaparin (Lovenox) therapy.
- Apply ice packs as indicated.
- Rationale: Promotes vasoconstriction to reduce bleeding or tissue edema in surgical area and lessens perception of discomfort.
- Initiate and maintain extremity mobilization: ambulation, physical therapy, exercise and/or CPM device.
- Rationale: Increases circulation to affected muscles. Minimizes joint stiffness; relieves muscle spasms related to disuse.
Nursing Diagnosis
Deficient Knowledge
May be related to
- Lack of exposure/recall
- Information misinterpretation
Possibly evidenced by
- Questions/request for information, statement of misconception
- Inaccurate follow-through of instructions, development of preventable complications
Desired Outcomes
- Verbalize understanding of surgical procedure and prognosis.
- Correctly perform necessary procedures and explain reasons for the actions.
Nursing Interventions
- Review disease process, surgical procedure, and future expectations.
- Rationale: Provides knowledge base from which patient can make informed choices.
- Encourage alternating rest periods with activity.
- Rationale: Conserves energy for healing and prevents undue fatigue, which can increase risk of injury or falls.
- Stress importance of continuing prescribed exercise and/or rehabilitation program within patient’s tolerance: crutch, cane walking, weight-bearing exercises, stationary bicycling, or swimming.
- Rationale: Increases muscle strength and joint mobility. Most patients will be involved in formal rehabilitation and/or outpatient home care programs or be followed in extended-care facilities by physical therapists. Muscle aching indicates too much weight bearing or activity, signaling a need to cut back.
- Instruct in home use of CPM exercise program.
- Rationale: CPM therapy may be continued for some patients after discharge. Note: CPM therapy is used in only about 50% of patients at this time.
- Review activity limitations, depending on joint replaced, for hip/knee sitting for long periods or in low chair/ toilet seat/ recliner, jogging, jumping, excessive bending, lifting, twisting or crossing legs.
- Rationale: Prevents undue stress on implant. Long-term restrictions depend on individual situation or physician’s protocol.
- Discuss need for safe environment in home (removing scatter rugs and unnecessary furniture) and use of assistive devices (handrails in tub or toilet, raised toilet seat, cane for long walks).
- Rationale: Reduces risk of falls and excessive stress on joints.
- Review and have patient or caregiver demonstrate incisional/wound care.
- Rationale: Promotes independence in self-care, reducing risk of complications.
- Identify signs and symptoms requiring medical evaluation, e.g., fever and chills, incisional inflammation, unusual wound drainage, pain in calf or upper thigh, or development of―strep throat or dental infections.
- Rationale: Bacterial infections require prompt treatment to prevent progression to osteomyelitis in the operative area and prosthesis failure, which could occur at any time, even years later.
- Review drug regimen: anticoagulants or antibiotics for invasive procedures.
- Rationale: Prophylactic therapy may be necessary for a prolonged period after discharge to limit risk of thromboemboli or infection. Procedures known to cause bacteremia can result in osteomyelitis and prosthesis failure.
- Notify of bleeding precautions. Instruct use of soft toothbrush, electric razors, avoidance of trauma or forceful blowing of the nose.
- Rationale: Reduces risk of therapy-induced bleeding and/or hemorrhage.
- Encourage intake of balanced diet, including roughage and adequate fluids.
- Rationale: Enhances healing and feeling of general well-being. Promotes bowel and bladder function during period of altered activity.
Other Nursing Care Plan Source
