Notes

Description
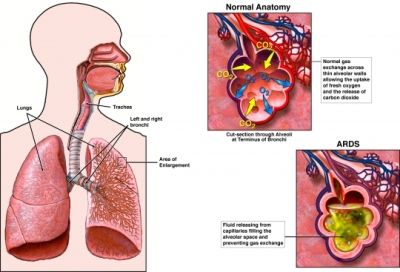
- Acute respiratory distress syndrome is a form of acute respiratory failure that occurs as a complication of some other condition, is caused by a diffuse lung injury, and leads to extravascular lung fluid.
- The major site of injury is the alveolar capillary membrane.
- The interstitial edema causes compression and obliteration of the terminal airways and leads to reduced lung volume and compliance.
- The ABG’s identify respiratory acidosis and hypoxemia that does not respond to an increase percentage of oxygen.
- The chest X-ray film shows interstitial edema.
- Some of the causes includes sepsis, fluid overload, shock, trauma, neurological injuries, burns, disseminated intravascular coagulation, drug ingestion and inhalation of toxic substances.
Causes & Risk Factors
ARDS can be caused by any major swelling (inflammation) or injury to the lung. Some common causes include:
- Breathing vomit into the lungs (aspiration)
- Inhaling chemicals
- Pneumonia
- Septic shock
- Trauma
ARDS leads to a buildup of fluid in the air sacs. This fluid prevents enough oxygen from passing into the bloodstream.
The fluid buildup also makes the lungs heavy and stiff, and decreases the lungs’ ability to expand. The level of oxygen in the blood can stay dangerously low, even if the person receives oxygen from a breathing machine (mechanical ventilator) through a breathing tube (endotracheal tube).
ARDS often occurs along with the failure of other organ systems, such as the liver or the kidneys. Cigarette smoking and heavy alcohol use may be risk factors.
Assessment
- Tachypnea
- Dyspnea
- Decrease breath sounds
- Deteriorating gas levels
- Hypoxemia despite high concentration of delivered oxygen
- Decreased pulmonary compliance
- Pulmonary infiltrates
Diagnostic Evaluation
- Based on clinical criteria history of risk factors acute onset of respiratory distress bilateral pulmonary infiltrates absence of left heart failure and severe refractory hypoxemia.
- Chest X-ray shows bilateral infiltrates and pulmonary edema.
Primary Nursing Diagnosis
- Impaired gas exchange related to increased alveolar-capillary permeability, interstitial edema and decreased lung compliance
Other Diagnoses that may occur in Nursing Care Plans For ARDS
- Ineffective airway clearance
- Ineffective breathing pattern
- Activity intolerance
- Anxiety (specify level: mild, moderate, severe, panic)
- Risk for aspiration
Medical Management
- Identify and treat the underlying condition insure early detection; use aggressive supportive treatment; prevent infection ( intubation and mechanical ventilation).
- As disease progresses, use positive and expiratory pressure PEEP ( neuromuscular blocking agent such as pancuronium (pavulon and vecuronium) (norcuron) maybe used to paralyzed patient for easier ventilation.
- Monitor arterial blood gas values , pulse symmetry , and pulmonary function testing.
- Provide circulatory support; treat hypovolemia carefully ; avoid overload
- Provide adequate fluid management ; administer intravenous solutions
- Provide nutritional support; (35 to 45 kilocalories per kilogram daily)
- Pharmacologic therapy may include human recombinant interleukin-1 receptor antagonist, neutrophil inhibitors, pulmonary- specific vasodilators, surfactant replacement therapy, antisepsis agents, antioxidant therapy, and corticosteroids (late in the course of ARDS).
Pharmacologic Intervention
- General Comments: Use of genetically engineered surfactant has been studied in ARDS but has not demonstrated the success that has occurred in premature infants with surfactant deficiency. Corticosteroids have been widely used in ARDS, yet studies have not consistently demonstrated any improvement in patient outcomes and remain controversial. Some evidence exists that prolonged treatment with low-dose corticosteroids may benefit patients with unresolving ARDS, particularly by reversing the process of fibroproliferation. If the patient is difficult to ventilate, she or he may receive skeletal muscle relaxants such as vecuronium (Norcuron), which are neuromuscular-blocking agents that paralyze the patient’s skeletal muscles. These medications are used only when the patient’s gas exchange is so poor as to threaten his or her life. Neuromuscular-blocking agents paralyze the patient without affecting mental status, so the patient requires sedation to counteract the accompanying fear and anxiety that occur when the patient is unable to move.
- Nitric oxide Inhalation route a pulmonary vascular vasodilator to decreases pulmonary vascular resistance with increased perfusion to ventilated areas
Nursing Intervention
- Identify and treat cause of the Acute respiratory distress syndrome
- Administer oxygen as prescribed.
- Position client in high fowler’s position.
- Restrict fluid intake as prescribed.
- Provide respiratory treatment as prescribed.
- Administer diuretics, anticoagulants or corticosteroids as prescribed.
- Prepare the client for intubation and mechanical ventilation using PEEP.
Documentation Guidelines
- Respiratory status of the patient: respiratory rate, breath sounds, and the use of accessory muscles; arterial blood gas (ABG) levels; pulse oximeter and chest x-ray results
- Response to treatment, mechanical ventilation, immobility, and bedrest
- Presence of any complications (depends on the precipitating condition leading to ARDS)
Discharge and Home Healthcare Guidelines
- PREVENTION. Prompt attention for any infections may decrease the incidence of sepsis,which can lead to ARDS.
- COMPLICATIONS. If patients survive ARDS, few residual effects are seen. Complications are directed to any other conditions the patient may have.
Sources:
ADAM for images
Marilyn Sawyer Sommers, RN, PhD, FAAN , Susan A. Johnson, RN, PhD, Theresa A. Beery, PhD, RN , DISEASES AND DISORDERS A Nursing Therapeutics Manual, 2007 3rd ed
Nursing crib.com
Handbook for Brunner & Suddarth’s, Textbook of Medical-SurgicalNursing, 11th ed
Exam
Nursing Care Plan
Nursing Diagnosis
- Ineffective Airway Clearance
- Ineffective Breathing Pattern
- Impaired Gas Exchange
- Decreased Cardiac Output
- Risk for Injury
- Excess Fluid Volume
- Impaired Physical Mobility
- Impaired Skin Integrity
- Impaired Verbal Communication
- Ineffective Coping
- Sleep Pattern Disturbance
 Nursing Management")

