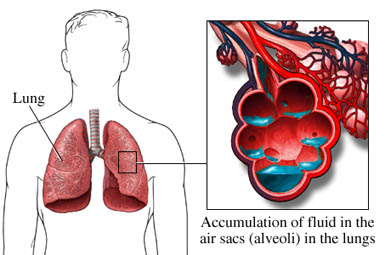
Description
Pulmonary edema is an abnormal accumulation of extravascular fluid as the lung parenchyma that interferes with adequate gas exchange. This is a life threatening situation that needs immediate treatment. The most common cause of cardiogenic pulmonary edema is left ventricular failure exhibited by increased left atrial ventricular pressures. Risk factors include ischemic heart disease, cardiomyopathy, valvular disease, myocardial infarction, and acute septal defects.
Signs And Symptoms
- Shortness of breath
- Orthopnea
- Moist cough with pink frothy sputum
- Chest discomfort
- Palpitations
- Fatigue
- Syncope
- Cyanosis
- Respiratory distress
Physical Examination
Appearance:
- Anxious
- Diaphoretic
- Clammy skin
Vital signs:
- HR: sustained tachycardia
- BP: < 90 mm Hg
- RR: > 30 breaths/minute
- Falling O2 saturations
Cardiovascular:
- Tachydysrhythmias with possible ectopy
- Laterally displaced point of maximal impulse (PMI)
- Murmur – mitral valve regurgitation
- S3 with possible S4
Pulmonary:
- Respiratory distress
- Respiratory failure
- Orthopnea
- Coarse bilateral crackles
- Wheezing
- Rhonchi
- Cough with frothy sputum
Acute Care Patient Management
Nursing Diagnosis: Impaired gas exchange related to increased pulmonary congestion secondary to increased left ventricular end diastolic pressure (LVEDP).
Outcome Criteria
- RR 12 to 20 breaths/min
- Eupnea
- Lungs clear to auscultation
- pH 7.35 to 7.45
- Pao2 80 to 100 mm Hg
- Paco2 35 to 45 mm Hg
- O2 sat ? 95%
- Svo2 60% to 80%
- P (a/A) O2 ratio 0.75 to 0.95
Nursing Interventions
Patient Monitoring
- Continuously monitor oxygenation status with pulse oximetry monitoring.
- Monitor ECG for dysrhythmia development that may be related to hypoxemia, acid-base imbalance, or ventricular irritability.
- Calculate arterial-alveolar oxygen tension ratio as an index of gas exchange efficiency.
- Document hourly the input and output to monitor fluid status. Obtain daily weights.
Patient Assessment
- Measure HR, RR, and BP every 15 minutes to evaluate the patient’s response to therapy and to detect cardiopulmonary deterioration.
- Assess the patient for changes that may indicate respiratory compromise, necessitating intubation and mechanical ventilation.
Diagnostic Assessment
- Review ABGs for hypoxemia (Pao2 < 60 mm Hg) and acidosis (pH < 7.35), which may further compromise tissue perfusion and to indicate need for mechanical ventilation.
- Review serial chest radiographs for worsening or resolving pulmonary congestion.
- Review lactate levels as an indicator of anaerobic metabolism.
Patient Management
- Provide supplemental oxygen via mask as indicated.
- Administer diuretic agents or nesiritide to reduce circulating volume, which will improve gas exchange.
- Monitor urine output and electrolytes.
- Administer vasodilating agents to redistribute fluid volumes, which will facilitate gas exchange.
- Morphine sulfate maybe ordered to promote preload and afterload reduction and to decrease anxiety.

