Notes
Definition
- Chronic pancreatitis is progressive pancreatic inflammation resulting in permanent structural damage to pancreatic tissue.
Risk Factors
- Repeated episodes of acute pancreatitis
- Alcoholism
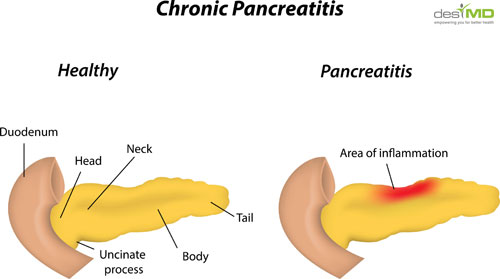
image courtesy of : desimd.com
Pathophysiology
- With repeated attacks of pancreatitis, pancreatic cells are progressively with fibrous tissue, causing increased pressure within the pancreas. Eventually, this results in mechanical obstruction of the pancreatic duct, common bile duct, and duodenum. Other effects include atrophy of the ductal epithelium, inflammation, and destruction of pancreatic cells.
Assessment/Clinical Manifestations/Signs and Symptoms
- Pain
- Weight loss
- Steatorrhea
- Anorexia
Laboratory and diagnostic findings.
- Serum amylase and lipase levels are elevated
- White blood cell count is elevated
- Endoscopic retrograde cholangiopancreatography detects pancreatic calcification.
- Glucose tolerance test values are abnormal.
Medical Management
Treatment is directed toward preventing and managing acute attacks.
- Pain and discomfort are relieved with analgesics.
- Patient should avoid alcohol and foods that produce abdominal pain and discomfort. No other treatment will relieve pain if patient continues to consume alcohol.
- Diabetes mellitus resulting from dysfunction of pancreatic islet of cells is treated with diet, insulin or oral hypoglycemic agents. Patient and family are taught the hazard of severe hypoglycemia related to alcohol use.
- Pancreatic enzyme replacement therapy is instituted for malabsorption and steatorrhea.
- Surgery is done to relive abdominal pain and discomfort, restore drainage of pancreatic secretions, and reduce frequency of attacks (pancreaticojejunostomy)
Nursing Diagnosis
- Chronic pain related to chronic pancreatitis
- Nutrition imbalance: less than body requirements, related to chronic pancreatitis
- Knowledge deficit related to chronic pancreatitis
Nursing Management
Promote measures to provide comfort.
- Provide symptomatic treatment, focusing on relieving pain, promoting comfort and treating new attacks.
- Emphasize the importance of avoiding alcohol, caffeine, and foods that tend to cause abdominal discomfort.
Prepare the client for surgery to relieve pain and drain cysts, if indicated.
Manage any endocrine insufficiency, such as diabetes mellitus, by initiating dietary and insulin or oral hypoglycemic therapy.
Administer prescribed medications, which include pancreatic enzymes, nonopioid pain medications, antacids, histamine receptor antagonists, and proton-pump inhibitors.
Nursing Care Plan
Nursing Diagnosis: Imbalanced Nutrition: Less Than Body Requirements
May be related to
- Vomiting, decreased oral intake; prescribed dietary restrictions
- Loss of digestive enzymes and insulin (related to pancreatic outflow obstruction or necrosis/autodigestion)
Possibly evidenced by
- Reported inadequate food intake
- Aversion to eating, reported altered taste sensation, lack of interest in food
- Weight loss
- Poor muscle tone
Desired Outcome
- Demonstrate progressive weight gain toward goal with normalization of laboratory values
- Experience no signs of malnutrition.
- Demonstrate behaviors, lifestyle changes to regain and/or maintain appropriate weight.
Nursing Interventions
- Assess abdomen, noting presence and character of bowel sounds, abdominal distension, and reports of nausea.
- Rationale: Gastric distention and intestinal atony are frequently present, resulting in reduced and absent bowel sounds. Return of bowel sounds and relief of symptoms signal readiness for discontinuation of gastric aspiration (NG tube).
- Provide frequent oral care.
- Rationale: Decreases vomiting stimulus and inflammation and irritation of dry mucous membranes associated with dehydration and mouth breathing when NG is in place.
- Assist patient in selecting food and fluids that meet nutritional needs and restrictions when diet is resumed.
- Rationale: Previous dietary habits may be unsatisfactory in meeting current needs for tissue regeneration and healing. Use of gastric stimulants (caffeine, alcohol, cigarettes, gas-producing foods), or ingestion of large meals may result in excessive stimulation of the pancreas and recurrence of symptoms.
- Observe color, consistency and amount of stools. Note frothy consistency and foul odor.
- Rationale: Steatorrhea may develop from incomplete digestion of fats.
- Note signs of increased thirst and urination or changes in mentation and visual acuity.
- Rationale: May warn of developing hyperglycemia associated with increased release of glucagon (damage to [beta] cells) or decreased release of insulin (damage to [beta] cells).
- Test urine for sugar and acetone.
- Rationale: Early detection of inadequate glucose utilization may prevent development of ketoacidosis.
- Maintain NPO status and gastric suctioning in acute phase.
- Rationale: Prevents stimulation and release of pancreatic enzymes (secretin), released when chyme and HCl enter the duodenum.
- Administer hyperalimentation and lipids, if indicated.
- Rationale: IV administration of calories, lipids, and amino acids should be instituted before nutrition and nitrogen depletion is advanced.
- Resume oral intake with clear liquids and advance diet slowly to provide high-protein, high-carbohydrate diet, when indicated.
- Rationale: Oral feedings given too early in the course of illness may exacerbate symptoms. Loss of pancreatic function and reduced insulin production may require initiation of a diabetic diet.
- Provide medium-chain triglycerides (MCTs) (MCT, Portagen).
- Rationale: MCTs are elements of enteral feedings (NG or J-tube) that provide supplemental calories and nutrients that do not require pancreatic enzymes for digestion and absorption.
Administer medications as indicated:
- Vitamins: A,D,E,K;
- Rationale: Replacement required because fat metabolism is altered, reducing absorption and storage of fat-soluble vitamins.
- Replacement enzymes: pancreatin (Dizymes), pancrelipase (Viokase, Cotazym).
- Rationale: Used in chronic pancreatitis to correct deficiencies to promote digestion and absorption of nutrients.
- Monitor serum glucose.
- Rationale: Indicator of insulin needs because hyperglycemia is frequently present, although not usually in levels high enough to produce ketoacidosis.
- Provide insulin as appropriate.
- Rationale: Corrects persistent hyperglycemia caused by injury to cells and increased release of glucocorticoids. Insulin therapy is usually short-term unless permanent damage to pancreas occurs.
Nursing Diagnosis: Deficient Knowledge
May be related to
- Lack of exposure/recall
- Information misinterpretation; unfamiliarity with information resources
Possibly evidenced by
- Questions, request for information; statement of misconception
- Inaccurate follow-through of instructions/development of preventable complication
Desired Outcomes
- Verbalize understanding of condition/disease process and potential complications.
- Verbalize understanding of therapeutic needs.
- Correctly perform necessary procedures and explain reasons for the actions.
- Initiate necessary lifestyle changes and participate in treatment regimen.
Nursing Interventions
- Review specific cause of current episode and prognosis.
- Rationale: Provides knowledge base on which patient can make informed choices.
- Discuss other causative and associated factors such as excessive alcohol intake, gallbladder disease, duodenal ulcer, hyper -lipoproteinemias, some drugs (oral contraceptives, thiazides, furosemide [Lasix], isoniazid [INH], glucocorticoids, sulfonamides).
- Rationale: Avoidance may help limit damage and prevent development of a chronic condition.
- Explore availability of treatment programs and rehabilitation of chemical dependency if indicated.
- Rationale: Alcohol abuse is currently the most common cause of recurrence of chronic pancreatitis. Usage of other drugs, whether prescribed or illicit, is increasing as a factor.Note: Pain of pancreatitis can be severe and prolonged and may lead to narcotic dependence, requiring need for referral to pain clinic.
- Stress the importance of follow-up care, and review symptoms that need to be reported immediately to physician (recurrence of pain, persistent fever, nausea and vomiting, abdominal distension, frothy and foul-smelling stools, general intolerance of food).
- Rationale: Prolonged recovery period requires close monitoring to prevent recurrence and complications (infection, pancreatic pseudocysts).
- Review importance of initially continuing bland, low-fat diet with frequent small feedings and restricted caffeine, with gradual resumption of a normal diet within individual tolerance.
- Rationale: Understanding the purpose of the diet in maximizing the use of available enzymes while avoiding overstimulation of the pancreas may enhance patient involvement in self-monitoring of dietary needs and responses to foods.
- Instruct in use of pancreatic enzyme replacements and bile salt therapy as indicated, avoiding concomitant ingestion of hot foods and fluids.
- Rationale: If permanent damage to the pancreas has occurred, exocrine deficiencies will occur, requiring long-term replacement. Hot foods and fluids can inactivate enzymes.
- Recommend cessation of smoking.
- Rationale: Nicotine stimulates gastric secretions and unnecessary pancreatic activity.
- Discuss signs and symptoms of diabetes mellitus (polydipsia, polyuria, weakness, weight loss).
- Rationale: Damage to the [beta] cells may result in a temporary or permanent alteration of insulin production.
