Definition
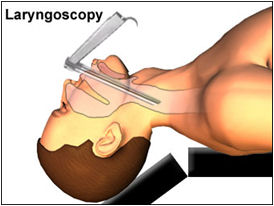
Direct laryngoscopy allows visualization of the larynx by the use of a fiberoptic endoscope or laryngoscope passed through the mouth or nose and pharynx and larynx. It’s indicated for any condition requiring direct visualization or specimen samples for diagnosis, such as in patients with strong gag reflexes resulting from anatomic abnormalities and in those who have had no response to short-term therapy for symptoms of pharyngeal or laryngeal disease, such as chronic hoarseness, stridor, and hemoptysis.
Secretions or tissue may be removed during this procedure for further study. The test is usually contraindicated in patients with epiglottitis, but it may be performed on them in an operating room with resuscitative equipment.
Purpose
- To detect lesions, strictures, or foreign bodies.
- To remove benign lesions or foreign bodies from the larynx.
- To help diagnose laryngeal or upper airway abnormalities.
- To examine the larynx when indirect laryngoscopy is inadequate.
Procedure
Preparation
- Make sure the patient has signed an appropriate consent form.
- Note and report all allergies.
- Check the patient’s history for hypersensitivity to the anesthetic.
- Instruct the patient to fast for 6 to 8 hours before the test.
- Give the patient a sedative to help him relax and a drug to reduce secretions.
- Give a general or local anesthetic to numb the gag reflex.
- Explain that the study takes about 30 minutes; it takes longer if minor surgery is performed as part of the procedure.
Implementation
- The patient is assisted into the supine position.
- A general anesthetic is given, or the mouth or nose and throat are sprayed with local anesthetic.
- The laryngoscope is inserted through the mouth.
- The larynx is examined for abnormalities.
- Specimens may be collected for further study.
- Minor surgery (polyp removal) may occur at this time.
Nursing Interventions
- Place the conscious patient in semi-Fowler’s position. Place the unconscious patient on his side with his head slightly elevated to prevent aspiration.
- Check the patient’s vital signs according to facility protocol, or every 15 minutes until the patient is stable and then every 30 minutes for 2 hours, every hour for the next 4 hours, and then every 4 hours for 24 hours.
- Immediately report to the practitioner any adverse reaction to the anesthetic or sedative such as tachycardia, palpitations, hypertension, euphoria, excitation, and rapid, deep aspirations.
- Apply an ice collar per institution protocol to minimize laryngeal edema.
- Provide an emesis basin, and instruct the patient to spit out saliva rather than swallow it.
- Observe sputum for blood, and report excessive bleeding immediately.
- Instruct the patient to refrain from clearing his throat and coughing to prevent hemorrhaging at the biopsy site.
- Advise the patient to avoid smoking until his vital signs are stable and there’s no evidence of comlications.
- Immediately report subcutaneous crepitus around the patient’s face and neck, which may indicate tracheal perforation.
- Listen to the patient’s neck with a stethoscope for signs of stridor and airway obstruction.
Interpretation
Normal Results
- No inflammation, lesions, strictures, or foreign bodies are found.
Abnormal Results
- Combine with the results of a biopsy, abnormal lesions suggest possible laryngeal cancer or benign lesions.
- Narrowing suggests stricture.
- Inflammation suggests possible laryngeal edema secondary to radiation or tumor.
- Asynchronous vocal cords suggest possible vocal cord dysfunction.
Complications
- Subcutaneous crepitus around the patient’s face and neck – a sign of tracheal perforation.
- Airway obstruction in the patient with epiglottiditis.
- Adverse reaction to anesthetic.
- Bleeding.
image by: privatehealth.co.uk
