Description
Hepatic failure can result from acute liver injury, causing acute liver failure (ALF) or fulminant hepatic failure (FHF), or progressive chronic liver disease such as cirrhosis. An alteration in hepatocyte functioning affects the liver metabolism, detoxification process, protein synthesis, manufacture of clotting factors, and preservation of immunocompetence. FHF occurs when severe hepatic injury results in encephalopathy and severe coagulopathy within 28 days of the onset of symptoms in patients without a history of chronic liver disease. Liver transplant is the only viable treatment option for patient with FHF. The most commonly identified cause of FHF is drug induced, with acetaminophen the most common culprit, followed by viral hepatitis. Other causes include infection (cytomegalovirus [CMV], adenovirus), metabolic disorders and severe ischemic insult or shock.
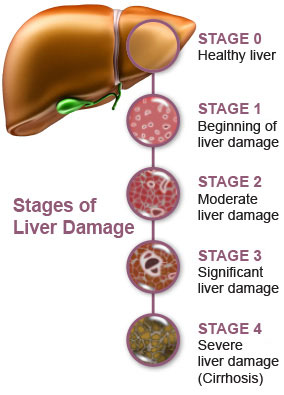
image by: http://vitaltherapies.com/
Signs and Symptoms
- Manifestation depends on the complications associated with the liver dysfunction.
- Patient behavior may range from agitation to frank coma.
- Evidence of GI bleeding, renal failure, or respiratory distress may also be present.
- The initial manifestation in FHF is commonly bleeding from coagulopathy.
Physical Examination
Vital signs
- BP: < 90 mm Hg (with shock)
- HR: > 120 beats/min (with shock)
- Temperature may be mildly elevated
- RR: tachypnea initially progressing to respiratory depression associated with encephalopathy.
Neurologic
- Mildly confused to coma
- Personality changes
- Asterixis
Pulmonary
- Crackles
- Labored respirations
Gastrointestinal
- Hematemesis and melena
- Ascites
- Hepatomegaly may be present
- Splenomegaly may be present
- Factor hepaticus
- Diarrhea
Skin
- Jaundice
- Ecchymosis and petechiae
- Pruritus
- Edema
Acute Care Patient Management
Nursing Diagnosis: Deficient fluid volume related to ascites secondaryto hypoalbumineia, bleeding secondary to decreased clotting factors or variceal hemorrhage, and diuretic therapy.
Outcome Criteria
- BP 90 TO 120 mm Hg
- Central venous pressure 2 to 6 mm Hg
- Serum albumin 3.5 to 5 mg/dl
- Platelet count >50,000/mm3
- Urine output 30 ml/hr
- Serum sodium 135 to 145 mEq/L
- Serum potassium 3.5 to 5 mEq/L
- Intake approximates output
Patient Monitoring
- Obtain pulmonary artery pressure, central venous pressure, and blood pressure until the patient’s condition is stable, then hourly.
- Continuously monitor ECG for lethal dysrhythmias that may result from electrolyte and acid-base imbalances.
- Monitor fluid volume status. Measure intake and output hourly.
Patient Assessment
- Assess hydration status. Note skin turgor on inner thigh or forehead, condition of buccal memranes, and development of edema and crackles.
- Assess for signs and symptoms of bleeding.
- Measure abdominal girth once each shift to determine progression of ascites.
- Assess respiratory status.
Diagnostic Assessment
- Review serial serum ammonia, albumin, bilirubin, platelet count, PT, PTT and ALT to evaluate hepatic function.
- Review serial serum electrolytes.
- Review urine electrolyte, BUN, and creatinine to evaluate renal function.
Patient Management
- Administer intravenous crystalloids as ordered.
- Administer potassium as ordered. Validate adequate urine output before potassium administration.
- Sodium restriction of 0.5 g/day and fluid restriction to 1000 ml/day may be ordered.
- Vitamin K or fresh frozen plasma (FFP) may be required to promote the clotting process.
- Institute bleeding precautions. Avoid razor blades and use soft-bristled toothbrushes.
- Paracentesis may be performed if abdominal distention is severe.
- Prepare the patient and family for liver transplant, as indicated.


