Description
Arteriovenous are malformation of the cerebrovascular system in which tortuous, tangled, and malformed arterial channels drain directly into the venous system without an intervening capillary bed. The arteries supplying the AVM tend to dilate with time as a result of increased flow through the lesion. The veins enlarge as the flow increases; creating a vicious cycle that can make this lesion increase in size. This large flow or shunting of the blood through the AVM can render adjacent areas (and sometimes distal areas) of the brain ischemic. The high flow state can lead to increased pressure and eventually hemorrhage, typically into the subarachnoid space and parenchymal tissue.
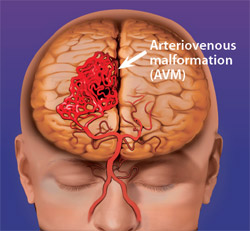
image credit to: http://webleed.org/
Signs and Symptoms
- Headache
- Seizures
- Syncope
- Progressive neurologic deficits
- Hemorrhage
Physical Examination
Vital signs:
- BP: Normotensive or hypertensive
- HR: Mild tachycardia may be present
- RR: Eupnea
Neurologic: depending on the area of the brain in which the AVM is located, there may be speech, motor, or sensory deficits. There also may be problems with vision, memory, and coordination.
Acute Care Patient Management
Nursing Diagnosis:
Ineffective tissue perfusion: Cerebral related to shunting of blood from cerebral tissue and/ or intracerebral hemorrhage (ICH).
Outcome Criteria
- Alert and oriented
- Pupils equal and normoreactive
- BP 90 to 140 mmHg
- HR 60 to 100 beats/minute
- RR 12 to 20 breaths/minute, eupnea
- Motor function equal bilaterally
- Absence of headache, nystagmus, and nausea
- Intracranial pressure (ICP) <20 mm Hg
- Cerebral perfusion pressure (CPP) 60 to 100 mm Hg
Nursing Interventions
Patient Monitoring
- Monitor ECG continuously because hypoxemia and cerebral bleeding are risk factors for pronounced ST segment and T-wave changes and life-threatening dysrhythmias.
- Monitor ICP, analyze the ICP waveform, and calculate CPP every hour.
- Monitor BP and pulse every 15 to 30 minutes initially, then hourly.
- Obtain CVP and/ or PA pressures if available, every hour or more frequently if indicated.
Patient Assessment
- Assess pain using the patient’s self-repot whenever possible.
- Note headache onset and severity; presence of stiff neck; and insidious onset of confusion, disoreintatio, decline in consciousness, and/or focal deficits (weakness of extremity).
- Assess neurologic status using Glascow Coma scale and assess for changes suggesting increased ICP and herniation.
- Be alert for subtle changes and new focal deficits.
- Assess for factors that can cause increased ICP, evaluate the patient for restlessness, distended bladder, constipation, hypovolemia, headache, fear, or anxiety.
Diagnostic Assessment
- Review serial ABGs for decreasing Pao2 (<60 mm Hg) or increasing Paco2 (.40 mm Hg) to identify causes for increased ICP.
Nursing Interventions
- Maintain patent airway and administer oxygen as ordered to prevent hypoxemia.
- Institute measures to minimize external stimuli and maintain BP level.
- Administer antihypertensive drugs as ordered. To control blood pressure.
- Sedatives and stool softeners may be prescribed to reduce agitation and straining.
- Anticipate interventions such as embolization, resection, clipping, ligation of feeding vessels, proton-beam therapy, or gamma radiation.
 Nursing Management & Care Plan")