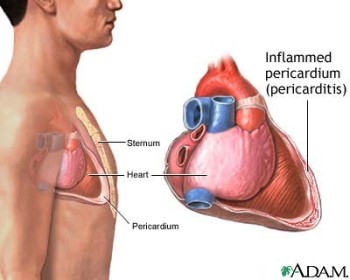
Description
Pericarditis is an inflammation and/ or infectious process of the pericardium, the sac that contains the heart. It may be an acute or chronic (constrictive) condition that can lead to pericardial effusion or tamponade. It can lead to arterial and ventricular dysrhythmias, limit the cardiac chamber’s ability to fill, and effect to cardiac output. Risk factors include bacterial and viral infections, vaasculitis – connective tissue disease, MI, uremia, neoplasms, and trauma; or can be iatrogenic (after cardiac surgery, drugs, and cardiac resuscitation) or idiopathic.
Signs And Symptoms
- Chest pain and fever are the most common manifestation.
- Pericardial friction rub is a clinical hall mark.
- Pain begins suddenly, is severe and sharp, and is aggravated by inspiration and deep breathing.
- Pain is usually anterior to the precordium, radiates to the left shoulder, and is generally relieved by sitting up and leaning forward.
Physical Examination
Appearance
- Restlessness
- Irritability
- Weakness
- Pallor
Vital signs
- HR: increased
- Temp: normal to increased
- RR: increased
Cardiovascular
- Friction rub
- Pulsus paradoxus
- Jugular vein distention
Acute Care Patient Management
Nursing Diagnosis: Ineffective breathing pattern related to acute painsecondary to inflammation and aggravated by position and inspiration.
Outcome Criteria
- Patient communicates pain relief
- Patient breathes with comfort
- O2 sat ? 92%
- RR 12 to 20 breaths/min, eupnea
Patient Monitoring
- Assess pain using patients self-report when possible. A self-report rating scale assesses intensity of pain.
- Auscultate the anterior chest to determine the quality of the friction rub.
- Assess respiratory status because the patient may hypoventilate as a result of pain.
Diagnostic Assessment
- Review the ABGs to evaluate oxygenation and acid-base status.
- Review results of echocardiogram and chest X-ray if available.
- Review serial ECGs for changes.
- Review CBC, leukocyte counts, and culture if possible.
Patient Management
- Administer pharmacologic agents such as ibuprofen and indomethacin, as ordered to reduce inflammation and pain.
- Stay with the patient, providing a calm, quiet environment.
- Assist the patient to maintain a position of comfort.
- Ensure activity restrictions while the patient is asymptomatic, febrile, or if friction rubs is present.
- Promote pulmonary hygiene to prevent risk of atelectasis.

