
Description
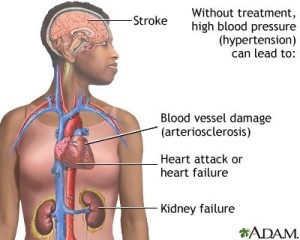
Hypertensive crisis is an emergent situation in which a marked elevation in diastolic blood pressure can cause end-organ damage. Severe hypertension, usually a diastolic reading >120 mm Hg can cause irreversible injury to the brain, heart, and kidneys that can rapidly lead to death. Hypertensive crisis can occur in patients with either essential hypertension (unknown) or secondary hypertension which can be a result of renal or endocrine disease. Emergencies include hypertension in association with acute central nervous system events, acute aortic dissection, pulmonary edema, pheochromocytoma crisis, eclampsia, and nonadherence to medical therapy.
Signs And Symptoms
- Headache
- Nausea
- Dizziness
- Visual disturbances
- Altered level of consciousness
Physical Examination
- BP >120 mm Hg
Acute Care Patient Management
Nursing Diagnosis: Ineffective tissue perfusion related to compromised blood flow secondary to severe hypertension resulting in end-organ damage.
Outcome Criteria
- Patient alert and oriented
- Skin warm and dry
- Pulses strong and equally bilaterally
- Capillary refill <3 sec
- BP <140 mm Hg
- BP < 90 mm Hg
- Mean arterial pressure 70 to 120 mm Hg
- HR 60 to 100 beats/min
- Absence of life-threatening dysrhythmias
- Urine output 30 mL/hr or 0.5 to 1 ml/kg/hr
- BUN <20 mg/dL, creatinine <1.5 mg/dL
Patient Monitoring
- Monitor arterial BP continuously and note sudden increases or decrease in readings. A precipitous drop in BP can cause reflex ischemia to the heart, brain, kidneys, and/or GI tract. Note trends in mean arterial pressure and the patient’s response to therapy.
- Monitor hourly urine output and note any presence of blood in the urine.
- Continuously monitor the ECG fir dysrhythmias or ST segment and T-wave changes associated with ischemia or injury.
Patient Assessment
- Assess the patient for laboratories indicated.
Diagnostic Assessment
- Review BUN and creatinine to evaluate the effect of BP on kidneys. BUN>20 mg/dL and creatinine >1.5 mg/dL suggest renal impairment.
- Review serial chest radiography for pulmonary congestion.
- Review serial 12-lead ECGs for patterns of injury, ischemia, and infarction
Patient Management
- Provide oxygen at 2 to 4 liters/min to maintain or improve oxygenation.
- Minimize oxygen demand by maintaining the patient at bed rest.
- Help the patient decrease anxiety, and keep the patient NPO or provide a liquid diet in the acute phase.
- Administer nitrates as ordered to reduce preload and afterload.
- Administer ?-blockers as ordered. Labetalol may be given as 20 to 80 mg bolus every 10 to 15 minutes to rapidly lower the blood pressure.
- Prepare the patient and family for surgical intervention to correct the underlying cause, if this is indicated.

