
Description
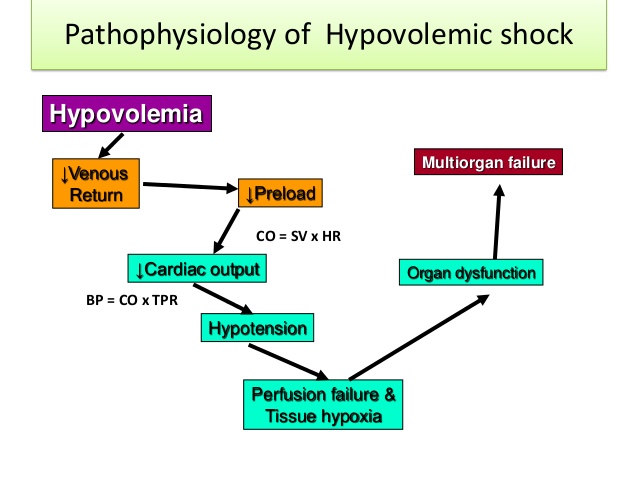
Hemorrhage is a major cause of hypovolemic shock. However, plasma loss/ dehydration and interstitial fluid accumulation (third spacing) adversely reduce circulating volume by decreasing tissue perfusion. The primary defect is decreased preload.
Four classifications of hypovolemic shock based on the amount of fluid and blood loss:
- Class I: <750 ml, or ? 15% total circulating volume.
- Class II: 750 to 1000 ml, 05 15% to 30% total circulating volume
- Class III: 1500 to 2000 ml, or 30% to 40% total circulating volume
- Class IV: >2000 ml, or > 40% total circulating volume. The patient’s compensatory response intensifies as the percent of blood loss is increases.
Signs And Symptoms
- Depends on the degree of blood loss and compensatory response.
Physical Examination
Appearance
- Anxiety progressing to coma
Vital signs
- Blood pressure normal to unobtaionable
- Palpable radial pulse reflects systolic blood pressure of 80 mm Hg
- Palpable femoral pulse reflects systolic blood pressure of 70 mm Hg
- Palpable carotid pulse reflects systolic blood pressure of 60 mm Hg
- HR normal to > 140 beats/min
- RR normal to > 35 breaths/ min
Cardiovascular
- Weak
- Thready pulse
Pulmonary
- Deep or shallow rapid respirations
- Lungs usually clear
Skin
- Cool, clammy skin, pale color
- Delayed/ absent capillary refill
- Lips cyanotic (late sign)
Acute Care Patient Management
Nursing Diagnosis: Ineffective tissue perfusion related to blood loss and hypotension.
Outcome Criteria
- Patient alert and oriented
- Skin warm and dry
- Peripheral pulses strong
- Urine output 30 ml/hr or 0.5 to 1 ml/kg/hr
- Hct – 32%
- Systolic blood pressure 90 to 120 mm Hg
- Mean arterial pressure 70 to 105 mm Hg
- Cardiac index 2.5 to 4 l/min/m2
- O2 sat ?95 %
Patient Monitoring
- Monitor BP continuously via arterial cannulation because cuff pressures are less accurate in shock states.
- Obtain cardiac output and cardiac index at least every 8 hours or more frequently to evaluate the patient’s response to changes in therapy.
- Monitor peripheral artery pressures and central venous pressure hourly or more frequently to evaluate the patient’s response to treatment.
- Continuously monitor ECG to detect life-threatening dysrythmias of HR > 140 beats/min, which can adversely affect SV.
- Monitor hourly urine output to evaluate renal perfusion.
- Measure blood loss if possible.
Patient Assessment
- Obtain vital signs every 15 minutes to evaluate the patient’s response to therapy and to detect cardiopulmonary deterioration.
- Assess level of consciousness, mentation, skin temperature, and peripheral pulses to evaluate tissue perfusion.
- Assess for pressure ulcer development.
Diagnostic Assessment
- Review Hgb and Hct levels and note trends. Decreased RBCs can adversely affect oxygen carrying capacity.
- Review lactate levels, an indicator of reduced tissue perfusion and anaerobic metabolism.
- Review ABGs for hypoxemia and respiratory or metabolic acidosis.
- Review BUN, creatinine, and electrolytes and more trends to evaluate renal function.
Patient Management
- Use a large bore (16 to 18 gauge) cannula for intravenous lines to replace volume rapidly.
- Administer blood products or autotranfuse as ordered.
- Administer colloids and crytalloids in addition to blood products as ordered.
- Pharmacologic agents may be used to improve hemodynamic parameters if intravascular volume is replaced.
- Provide oxygen as ordered.
- Prepare the patient for surgical intervention is required.
- Institute pressure ulcer prevention strategies.
