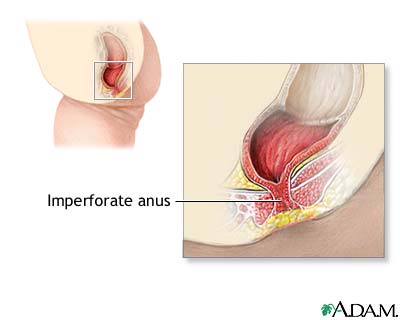
Definition
The establishment of colorectal continuity when there is absence of an anal orifice, and/ or closure of fistula if present.
Discussion
There are four classes or description of imperforate anus:
- Stemosis of the anus or distal rectum- treated by dilation and/ or incision.
- Membranous barrier at the anal opening – treated with incision and dilation.
- Rectum ends in a blind pouch above the perineum, usually associated with various fistulas. Correction will depend on the pathology present.
- Anal canal and distal rectum end in a blind pouch proximally. The more proximal rectum ends in a blind pouch above the distal segment.
- Type IV is a rare and usually treated by a preliminary colostomy, with a second-stage repair several months later.
- Type III may also be initially treated with a colostomy, with definitive repair occurring around three months of age depending on the child’s general health status.
Positioning
- Modified lithotomy or supine with frog-leg-like position.
- A folded towel is placed under the buttocks to elevate anal area.
Packs/ Drapes
- Pediatric lap sheet with extra fenestration created for combined approach.
- Peadiatric lap sheet with abdominal opening covered and hole created for a perineal approach.
Instrumentation
- Pediatric laparotomy tray
- Hegar dilators
Supplies/ Equipment
- Thermal blanket
- Handheld cautery
- Suction
- Scale
- Basin set
- Blades
- Needle counter
- Nerve stimulator
Procedure Overview
Imperforate Anus Class III
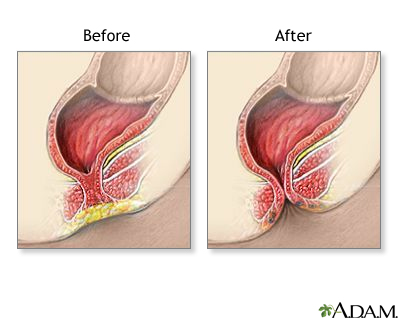
- Identification of the tract is accomplished using a small clamp inserted into the fistula.
- A perinea incision is then made in the midline of the tract.
- Dissection carried through the skin and subcutaneous tissue.
- The fistula is identified and divided; the exterior end is not closed, to allow postoperative drainage.
- The rectum is freed on all sides and the rectoanal repair is started using absorbable sutures.
- The rectum is opened and the bowel wall is trimmed back.
- Traction sutures are placed through the skin and the full thickness of bowel.
- Repeated dilation may be necessary as the opening may shrink in the next few months.
Perioperative Nursing Consideration
- Check with blood bank for available units.
- Maintain aseptic technique during perineal portion of the procedure.
- If tape is used during positioning, do not allow tape to directly contact the skin.
- Obtain and segregate specimens for multiple biopsies in separate containers as needed.
image by:nlm.nih.gov


