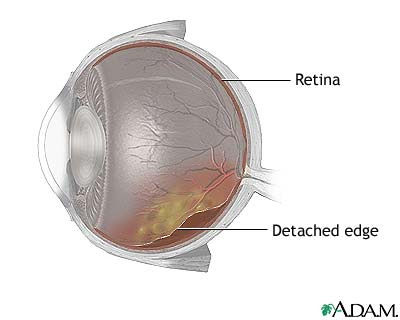
Description
- Results from separation of the sensory layer of the retina containing the rod and cones from the pigmented epithelial layer beneath.

- It may occur spontaneously because of degenerative changes in the retina (as in diabetic retinopathy) or vitreous humor, trauma, inflammation, tumor, or loss of a lens to a cataract.
- It is rare in children, the disorder most commonly occurs after age 40.
- Untreated retinal detachment results in loss of a portion of the visual field.
Causes/Risk factors
Modifiable
- Trauma
- Hemorrhage
- Exudates that occur in front of or behind the retina
- Sudden, severe physical exertion especially in persons who are debilitated.
Non-modifiable
- Myopic degeneration
- Aphakia (absence of crystalline lens)
Assessment
- Initially, the patient complains of flashes of light, floating spots or filaments in the vitreous, or blurred, “sooty” vision. Most of these phenomena result from traction between the retina and vitreous.
- If detachment progresses rapidly, the patient may report a veil-like curtain or shadow obscuring portions of the visual field. The veil appears to come from above, below, or from one side; the patient may initially mistake the obstruction for a drooping eyelid or elevated cheek.
- Straight-ahead vision may be unaffected in early stages but, as detachment progresses, there will be loss of central as well as peripheral vision.
Diagnostic Evaluation
- Ophthalmoscopy or slit-lamp examination with full pupil dilation shows retina as gray or opaque in detached areas. The retina is normally transparent.
Primary Nursing Diagnosis
- Sensory-perceptual alterations (visual) related to decreased sensory reception
Medical Management
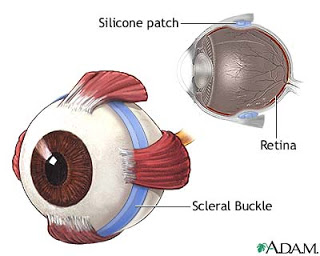
- Surgical intervention aims to reattach the retinal layer to the epithelial layer and has a 90% to 95% success rate.
Techniques include:
- Photocoagulation, in which a laser or xenon are “spot welds” the retina to the pigment epithelium.
- Electrodiathermy, in which a tiny hole is made in the sclera to drain subretinal fluid, allowing the pigment epithelium to adhere to the retina.
- Cryosurgery or retinal cryopexy, another “spot weld” technique that uses a super cooled probe to adhere the pigment epithelium to the retina.
- Scleral buckling, in which the sclera is shortened to force the pigment epithelium closer to the retina; commonly accompanied by vitrectomy.
Pharmacologic Intervention
- Drops as prescribed of Cyclopentolate hydrochloride (Cyclogyl) a cycloplegic agent that causes dilation of the pupil and rest of the muscles of accommodation
- Drops as prescribed of antibiotics Gentamicin; prednisolone acetate to prevent eye infections
- Other Drugs: Antiemetics and analgesics are ordered to manage nausea, vomiting, and pain.
Nursing Intervention
- Prepare the patient for surgery.
- Instruct the patient to remain quiet in prescribed (dependent) position, to keep the detached area of the retina in dependent position.
- Patch both eyes.
- Wash the patient’s face with antibacterial solution.
- Instruct the patient not to touch the eyes to avoid contamination.
- Administer preoperative medications as ordered.
- Take measures to prevent postoperative complications.
- Caution the patient to avoid bumping head.
- Encourage the patient no to cough or sneeze or to perform other strain-inducing activities that will increase intraocular pressure.
- Encourage ambulation and independence as tolerated.
- Administer medication for pain, nausea, and vomiting as directed.
- Provide quiet diversional activities, such as listening to a radio or audio books.
- Teach proper technique in giving eye medications.
- Advise patient to avoid rapid eye movements for several weeks as well as straining or bending the head below the waist.
- Advise patient that driving is restricted until cleared by ophthalmologist.
- Teach the patient to recognize and immediately report symptoms that indicate recurring detachment, such as floating spots, flashing lights, and progressive shadows.
- Advise patient to follow up.
Documentation Guidelines
- Visual acuity
- Reaction to activity restrictions; ability of patient to participate in activities of daily living independently
- Complications such as bleeding,infection,decreased visual acuity,falls
- Response to medications and ability of the patient to instill eye drops
- Understanding of eye care at home
Discharge and Home Healthcare Guidelines
- Have the patient or significant others demonstrate the correct technique for instilling eye drops. Instruct the patient to wash her or his hands before and after removing the dressing; using a clean washcloth, cleanse the lid and lashes with warm tap water; tilt the head backward and inclined slightly to the side, so the solution runs away from the tear duct and other eye to prevent contamination; depress the lower lid with the finger of one hand. Tell the patient to look up when the solution is dropped on the averted lower lid; do not the place drop directly on the cornea.
- Do not touch any part of the eye with the dropper; close the eye after instillation, and wipe off the excess fluid from the lids and cheeks. Close the eye gently so the solution stays in the eye longer.
- Teach the patient to use warm or cold compresses for comfort several times a day. Note that the patient should wear either an eye shield or glasses during the day, during naps, and at night.
- Teach the patient to avoid vigorous activities and heavy lifting for the immediate postoperative period.
- Teach the patient the symptoms of retinal detachment and the action to take if it occurs again.
- Instruct the patient about the importance of follow-up appointments,which may be every few days for the first several weeks after surgery.
Sources:
Marilyn Sawyer Sommers, RN, PhD, FAAN , Susan A. Johnson, RN, PhD, Theresa A. Beery, PhD, RN , DISEASES AND DISORDERS A Nursing Therapeutics Manual, 2007 3rd ed
UDAN, Mastering Medical-Surgical Nursing


