Notes
Description
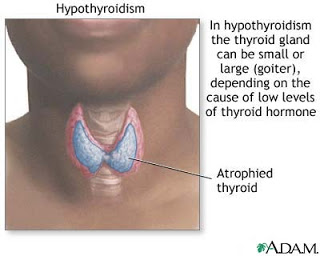
- Hypothyroidism is a hypothyroid state resulting from a hyposecretion of the thyroid hormones T4 and T3.
- Hypothyroidism is characterized by decreased rate of body metabolism.
Causes
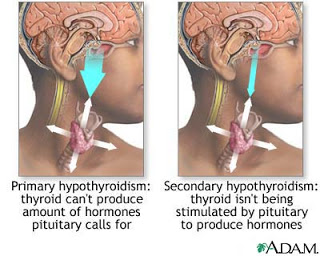
- Hypothyroidism can be a primary disorder that results from disease in the thyroid gland itself or a secondary or tertiary disorder. In most cases, hypothyroidism occurs as a primary disorder and results from the loss of thyroid tissue, which leads to inadequate production of thyroid hormones (primary hypothyroidism). It is most frequently autoimmune in origin but can also be related to iodine deficiency.
- Secondary hypothyroidism, which occurs in only 5% of cases, is caused by a failure of the pituitary gland to stimulate the thyroid gland or a failure of the target tissues to respond to the thyroid hormones. Tertiary hypothyroidism is caused by failure of the hypothalamus to produce thyroid-releasing factor.
- The most common cause of goitrous hypothyroidism in North America is Hashimoto’s disease, which causes defective iodine binding and defective thyroid hormone production. Hashimoto’s disease is common in the same family and is considered an autoimmune disorder leading to chronic inflammation of the thyroid gland and hypothyroidism but can also lead to hyperthyroidism.
Risk Factors
- Age over 50 years
- Being female
Assessment
- Lethargy and fatigue
- Weakness, muscle aches, paresthesias
- Intolerance to cold
- Weight gain
- Dry skin and hair
- Loss of body hair
- Bradycardia
- Constipation
- Generalized puffiness and edema around the eyes and face.
- Forgetfulness and loss of memory
- Menstrual disturbances
- Cardiac enlargement, tendency to develop congestive heart failure.
Complications
Myxedema coma, the most severe form of hypothyroidism, is rare. It may be caused by an infection, illness, exposure to cold, or certain medications in people with untreated hypothyroidism.
Symptoms and signs of myxedema coma include:
- Below normal temperature
- Decreased breathing
- Low blood pressure
- Low blood sugar
- Unresponsiveness
Primary Nursing Diagnosis
- Activity intolerance related to weakness and apathy
Diagnostic Evaluation
- Thyroid-stimulating hormone (TSH) assay result is >4.0 mU/L ( normal values: 0.5–1.5 mU/L). Normal value excludes primary hypothyroidism and a markedly elevated value confirms the diagnosis.
- Thyroxine (T4) radioimmunoassay decreased (normal values: 5.0–12.0 μg/dL). Reflects underproduction of thyroid hormones; monitors response to therapy.
- Tri-iodothyronine (T3) radioimmunoassay decreased (normal values: 80–230 ng/dL). Reflects underproduction of thyroid hormones.
- Electrocardiogram (ECG) reveals low voltage, T wave abnormalities.
- Other Tests: 24-hr radioactive iodine uptake; thyroid autoantibodies; antithyroglobulin
Medical Management
- Most patients are diagnosed and treated on an outpatient basis. The goal of treatment is to return the patient to the euthyroid (normal) state and to prevent complications. The treatment of choice is to provide thyroid hormone supplements to correct hormonal deficiencies.
- Treatment of the elderly patient is approached more cautiously because of higher risk for cardiac complications and toxic effects. The medication should not be given if the pulse rate is greater than 100. The treatment is considered to be life-long, requiring ongoing medical assessment of thyroid function.
- Polypharmacy is a significant concern for the hypothyroid patient. Several classifications of drugs are affected by the addition of thyroid supplements, including beta blockers, oral anticoagulants, bronchodilators, digitalis preparations, tricyclic antidepressants, and cholesterol lowering agents.
- Because significant cardiovascular disease often accompanies hypothyroidism, the patient is at risk for cardiac complications if the metabolic rate is increased too quickly. Therefore, the patient needs to be monitored for cardiovascular compromise (palpitations, chest pain, shortness of breath, rapid heart rate) during early thyroid therapy. The diet for the hypothyroid patient is generally low in calories, high in fiber, and high in protein. As the metabolic rate rises, the caloric content can be increased. The patient’s intolerance to cold may extend to cold foods,making meal planning more difficult.
Pharmacologic Highlights
- Treatment consists of replacing the deficient hormone with synthetic thyroid hormone; low doses are initially used, and the dose is increased every 1 to 2 months based on the clinical response and serial laboratory measurements that show normalization of thyroid-stimulating hormone (TSH) levels in primary hypothyroidism. The patient begins to experience clinical benefits in 3 to 5 days, which level off after approximately 4 to 6 weeks. After the dose is stabilized, patients can be monitored with laboratory measurement of TSH annually.
- Levothyroxine sodium a synthetic thyroid hormone replacement is used to returns the patient to the euthyroid (normal) state. Dosage is 1.5–2.5 mcg/kg PO daily; (use lowest dose possible because over-replacement of thyroid can cause bone loss or cardiovascular complications).
Nursing Interventions
- Monitor vital signs, including heart rate and rhythm.
- Administer thyroid replacement, levothyroxine sodium (Synthroid) is most commonly prescribed.
- Instruct the client about thyroid replacement therapy.
- Instruct the client in low-calorie, low-cholesterol, low-saturated-fate diet.
- Assess the client for constipation; provide roughage and fluids to prevent constipation.
- Provide a warm environment for the client.
- Avoid sedatives and narcotics because of increase sensitivity to these medications.
- Monitor for overdose of thyroid medications, characterized by tachycardia, restlessness,, nervousness, and insomnia.
- Instruct the client to report episodes of chest pain immediately.
Documentation Guidelines
- Physical findings: Cardiovascular status, bowel activity, edema, condition of skin, and activity tolerance
- Response to medications, skin care regimen, nutrition
- Psychosocial response to changes in bodily function, including mental acuity
Discharge and Home Healthcare Guidelines
- Explain all medications, including dosage, potential side effects, and drug interactions. Instruct the patient to check the pulse at least twice a week and to stop the thyroid supplement and notify the physician if the pulse is greater than 100. Explain that the healthcare professional should be notified about the condition. Explain that ongoing medical assessment is required to check thyroid function and that the medications may lead to hyperthyroidism despite the patient’s underlying hypothyroidism.
- Teach the patient about the thyroid gland and hypothyroidism, as well as complications such as heart disease and edema. Teach the patient that new cardiac or hyperthyroidism symptoms need to be reported immediately. Explain that the caloric and fiber requirements vary. The patient should report any abnormal weight gain or loss or change in bowel elimination.
Exam
Nursing Care Plan
Nursing Care Plan for Hypothyroidism
Nursing Diagnosis
Disturbed Sensory Perception (specify: visual)r/t the transmission of sensory impulses as a result of ophthalmopathy.
Goal
- Patients did not experience a decrease in visual acuity worse and there is no trauma / injury to the eye.
Intervention
- Instruct the patient when sleeping with head elevation position.
- Rationale: To reduce trauma to the eye.
- Wet the eye with sterile water.
- Rationale: To provide comfort to the eye.
- If the patient can not close their eyes tightly while sleeping , use a non- allergic plaster.
- Rationale: Make it easy for the patient to sleep.
- Give steroid medications as ordered. In severe cases, doctors usually prescribe medications such as steroids to reduce edema and diuretics.
- Rationale: Reduce edema and fluid.
Nursing Diagnosis
Decreased cardiac output r / t changes in stroke volume.
Goal
- to remain cardiovascular function optimally characterized by blood pressure, and heart rhythm within normal limits.
Intervention
- Monitor blood pressure, heart rate and rhythm every 2 hours.
- Rationale: To indicate the likelihood of cardiac hemodynamic disturbances such as hypotension, decreased urine output , and mental status changes.
- Instruct the patient to notify the nurse immediately if the patient experiences chest pain.
- Rationale: Because in patients with hypothyroidism can develop chronic arteriosclerosis.
- Collaboration of drugs.
- Rationale: To reduce the symptoms.
- Teach the patient and family how to use drugs and the signs to look out for in case of hyperthyroidism due to excessive use of drugs.
- Rationale: To identify drug reaction that is given to the patient.
Nursing Diagnosis
Imbalance nutrition less than body requirements r / t anorexia.
Goal
- Nutrition can be met, with the following criteria: weight gain, good skin texture.
Intervention
- Encourage increased fluid intake.
- Rationale: To increase the intake of fluids in the body of the patient.
- Give foods rich in fiber.
- Rationale: To ensure adequate intake of nutrients in the body.
- Teach the patient, about the kinds of foods that contain lots of water.
- Rationale: In order for the patient to know about what foods are good to eat.
- Collaboration with a nutritionist.
- Rationale: For a given proper nutrition.
Nursing Diagnosis
Activity Intolerance r / t generalized weakness
Goal
- Patients can rest.
Intervention
- Set the time interval between rest and activity to improve exercise that can be tolerated.
- Rationale: To improve resting and exercise that can be tolerated.
- Help the patient self-care activities when the patient is in a state of fatigue.
- Rationale: To prevent decubitus sores.
- Give stimulation through conversation and activities that do not cause stress.
- Rationale: Aiming to avoid any stress.
- Monitor the patient’s response to increased activity.
- Rationale: To determine the development of the activity in patients.

