Description and Etiology
Central canal stenosis
The normally triangular-shaped spinal canal becomes flattened, compressing the thecal sac. As it progresses, the cauda equine is compressed. This can be caused by any of the following, or any combination of the following:
- facet hypertrophy
- thickening and bulging of the ligament flava
- outward disc bulging
- disc degeneration
- spondylosis
- degenerative spondylolisthesis. The condition is aggravated by positions of extension, which produce more central-canal and lateral-recess narrowing.
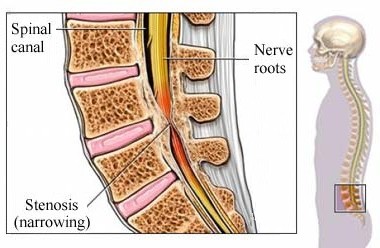
image by : http://fitstopphysicaltherapy.com/
Lateral-recess stenosis
Lateral-recess stenosis is a narrowing in the area where the nerve roots exit the spinal canal. It can also be caused by facet hypertrophy, disc bulging, loss of disc height, spondylosis, or degenerative spondylolisthesis.
Neurogenic claudication
Compression of the microvasculature of the lumbar nerve roots, resulting in ischemia and pain, is believed to be a major contributing factor in development of neurogenic claudication. In addition to ischemia, postural changes can cause stenosis. Postural neurogenic claudication is induced when the lumbar spine is extended and lordosis is accentuated, whether at rest or during exercise in the erect posture. With extension of the spine, degenerated intervertebral discs and thickened ligamenta flava protrude posteriorly into the lumbar canal, producing transient compression of the cauda equina. In the ischemic form, it is theorized that transient ischemia occurs in compressed lumbosacral roots when increased oxygen demand occurs during walking (Siebert, et al., 2009).
Definitions
- Congenital stenosis: The patient was born with a small narrow spinal canal.
- Acquired stenosis: The spinal canal has narrowed because of degenerative changes.
Incidence
A person with severe congenital lumbar stenosis may become symptomatic as early as age 20, whereas someone with acquired lumbar spinal stenosis becomes symptomatic at age 60–70.Males have a higher incidence than females. There does not appear to be any correlation between race and lumbar stenosis. Although L4–L5 is the most frequently involved level, lumbar stenosis may be found focally over one or two segments or at multiple levels.
Nursing Assessment, Interventions, and Monitoring
A. Preoperative
- Surgical procedure
- Preoperative history and physical
- Informed consent (obtained by surgeon)
- Anticipation of perioperative and postoperative care needs
- Initially, patient will need assistance and must arrange for a care provider.
- Patient should arrange for help with household chores, yard work, pets, and other tasks.
- Potential risks and complications
- Expected outcomes, both postoperative and long term
- Realistic patient expectations
- Mutual patient and physician expectations
- Required preoperative testing: For this patient population, special attention needs to be paid to preoperative medical clearance because of advanced age or other medical conditions.
- Discontinuation of medications, including herbal products, NSAIDs, anticoagulants, aspirin, warfarin, clopidogrel bisulfate
B. Perioperative
- Explain to patient where and when to arrive, as well as surgery time.
- Instruct patient on eating and drinking restrictions.
- Instruct patient on medications to be taken the morning of the surgery with a sip of water. Be aware of the institution’s anesthesia guidelines.
- Remind patient to wear comfortable clothing and to leave jewelry and valuables at home.
- Tell patient to remove dentures, partial plates, eyeglasses, contact lenses, nail polish, and sculptured nails.
C. Intraoperative
- Prone position is generally used.
- Patient’s abdomen should hang free to reduce intraoperative bleeding by minimizing vena cava compression and epidural venous pressure.
- Pressure points and genitalia should be checked to avoid positioning injuries.
- Lateral position is difficult.
D. Postoperative
- Neurological assessment
- Strength and sensation assessment should be compared with preoperative status.
- Pay special attention to the neurological assessment and correlation to the operative intervention.
- In the event of significant nerve root manipulation intraoperatively or neurological deficits postoperatively, the physician may order postoperative steroids for 24–48 hours. Antibiotics may be continued for 24 hours.
- Mobility
- Patient should mobilize quickly unless ordered differently due to complication (e.g., CSF leak).
- Instruct and help patient to roll to side and bring legs down while simultaneously rising up with the torso from the bed. This minimizes twisting at the waist.
- Instruct and help patient to rise from a chair using the legs, rather than pushing off with the back.
- Patient may benefit from a walker if he or she is deconditioned, had a multilevel laminectomy, or has difficult mobility.
- Evaluate the patient for need for an inpatient physical therapy referral for gait training and walker evaluation.
- Instruct patient to take short walks to avoid excessive fatigue; note preoperative walking endurance.
- If a CSF tear has occurred, physician may order flat bed rest. This is often dependent on degree of tear, ease of repair, and surgeon preference. For a persistent CSF leak, a lumbar drain may be implemented.
- Pain control
- The degree of pain varies considerably.
- Intravenous hydromorphone or morphine sulfate may be used as needed until the patient is able to take oral medications.
- Codeine, hydrocodone, or oxycodone, with or without acetaminophen, may be prescribed as needed when the patient is able to take oral medications.
- NSAIDs, as needed, can be very beneficial.
- Neuropathic pain medications (e.g., gabapentin) may be beneficial.
- Antispasmodics may be prescribed if muscle spasms are present.
- Heat may be applied for spasms and muscular tension.
- Ice may be applied for radicular pain for no more than 20 minutes per hour.
- Gentle massage may be used away from the incision.
- Have patient change positions frequently.
- Note geriatric considerations when administering medications.
- Constipation prevention
- Consider preoperative initiation.
- Ensure adequate water intake.
- Diet should include adequate fresh fruits, vegetables, and fiber.
- Stool softener (e.g., docusate) may be used 2-3 times per day.
- Motility agents (e.g., senna) should be used only as needed. Geriatric patients are prone to chronic constipation problems.
- Urination
- Urinary hesitancy, especially in the immediate postoperative period, is usually transient.
- Assess urinary output, frequency, and volume.
- Assess to be sure there is adequate emptying. Bladder scanning or intermittent bladder catheterization may be necessary to assess for retention or incomplete emptying. Patient may have long-standing urinary retention.
- Incision care
- Assess incision to be sure it is clean and dry.
- Care varies widely depending on the type of closure (staples, sutures, skin glue).
- In general, incision needs to be monitored daily for redness, drainage, and signs of infection. Patient and caregiver need to be instructed on specific incision care, evaluation for signs and symptoms of infection, and when and who to call with questions or problems.
- Postoperative teaching
- Avoid heavy lifting (anything heavier than a gallon of milk) for the first 4–6 weeks.
- Avoid prolonged sitting or standing for the first 4–6 weeks, including long car trips.
- The need for outpatient therapy is decided on individual basis.
- Patient will gradually be weaned from pain medication.
- Discharge planning
- Discharge planning should be initiated preoperatively.
- Talk to patient about how to gradually return to activities of daily living (ADLs) and lifestyle.
- Reinforce to patient the following: no lifting, bending, or twisting; no sitting for long periods of time.
- Remind patient to change positions frequently.
- Remind patient not to drive while using narcotic pain medications.
- Explain to patient that sexual activity may be resumed when it is comfortable.
- Ensure that the patient is aware of return-to-work and activity recommendations. Return to work will vary depending on type of work (sedentary roles earlier than heavy labor). Return to work may be a gradual progression to full time.
- Reinforce alternative planning and problem solving for practical everyday activities (e.g., vacuuming, doing laundry, performing child care).
- Explain incision care.
- Ensure that the patient is aware of postoperative follow-up recommendations.
- Patient comorbidities may affect postoperative recovery.