Nursing Assessment, Intervention, and Monitoring
Preoperative
- Surgical procedure
- Informed consent (obtained by surgeon)
- Expected outcomes (postoperative and long term)
- Required preoperative testing
- Discontinuation of medications (e.g., herbal products, NSAIDs, anticoagulants, aspirin, warfarin, clopidogrel bisulfate)
Perioperative
- Explain to patient where and when to arrive as well as surgery time.
- Instruct patient on eating and drinking restrictions.
- Instruct patient on medications to be taken the morning of the surgery with a sip of water.
- Remind patient to wear comfortable clothing and to leave jewelry and valuables at home.
- Remind patient to remove dentures, partial plates, eyeglasses, contact lenses, nail polish, and sculptured nails.
Intraoperative
- Plan for equipment needs
- Potential 3-D stereotactic guidance system
- Specialty table
- May need fluoroscope in room
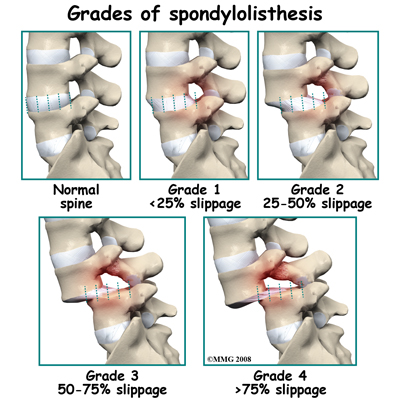
image by: http://www.eorthopod.com/
Postoperative
- Neurological assessment
- Strength and sensation assessment as compared with preoperative status
- Special attention to the neurological assessment and correlation to the operative intervention
- Patients with diabetes and obesity are at higher risk of postoperative complications, particularly wound infection. Measures to maintain glycemic control and deep vein thrombosis prophylaxis is particularly important in patients with these risk factors.
- Mobility
- Patient should mobilize quickly unless ordered differently due to complication (e.g., CSF leak).
- Instruct and help patient to roll to side and bring legs down while simultaneously rising from the bed with the torso. This minimizes twisting at the waist.
- Instruct and help patient to rise from a chair using the legs rather than the back.
- Bracing
- The decision whether to brace and the type of brace used to use varies widely.
- The decision is dependent on the surgery performed, bone quality, and physician preference.
- If braces are ordered, patient should be given specific guidelines regarding use.
- Pain control
- Methods to reduce postoperative pain vary according to clinical practice preferences. Patient-controlled analgesia (PCA) and patient-controlled epidural analgesia (PCEA) provide good overall patient satisfaction. The only clinical advantage of PCEA over PCA for spine fusion patients was the lower quantity of opioids consumed, although the PCEA group experienced significantly more side effects than the PCA group did. There were no other significant differences. Therefore, the patient or physician can select either postoperative pain management delivery system. Continuous epidural infusion of 0.1% ropivacaine resulted in lower pain scores, lower opioid consumption, and higher patient satisfaction when compared withplacebo (saline) in a study by Gottschalk and colleagues. Application of ropivacaine using an epidural catheter seems to be highly effective for postoperative pain after major lumbar spinal surgery. Postoperative continuous infusion of 0.5% marcaine into the subfascial aspects of the wound resulted in lower pain scores and less narcotic use in patients undergoing lumbar fusion compared to those receiving standard pain management. If postoperative pain is out of proportion and impairs activities, an X ray or CT scan, or both, of the lumbar spine should be considered to evaluate the screw location and to demonstrate integrity of the spinal canal. Other pain management options include the following: intravenous hydromorphone or morphine sulfate, as needed, until the patient is able to take oral medications; codeine, hydrocodone, or oxycodone, with or without acetaminophen, as needed, when the patient is able to take oral medications; antispasmodics, if muscle spasms are present; neuropathic pain medications (e.g., Gabapentin). Nonsteroidal anti-inflammatory drugs (NSAIDS) are typically avoided due to the possible interference with bone fusion.
Nutrition
- Patients are at high risk of developing a postoperative ileus.
- The timing of initial oral intake varies widely. In the fasting patient, the presence of bowel sounds may not reflect gastrointestinal motility when the patient eats. Regarding early postoperative eating and its effect on postoperative ileus, literature review found that early enteral feeding decreased the duration of postoperative ileus and length of stay. They noted that, because early feeding does not increase the occurrence of associated complications, it may be used as a strategy to prevent postoperative ileus.
Constipation prevention
- Consider initiating preoperatively.
- Ensure adequate water intake.
- Diet should include adequate fresh fruits, vegetables, and fiber.
- Stool softener (e.g., docusate) may be used two to three times per day.
- Motility agents (e.g., senna) should be used only as needed. ensure there is adequate emptying. Bladder scanning or intermittent bladder catheterization may be necessary to assess the patient for retention or incomplete emptying.
Discharge planning
- Discharge planning should be initiated preoperatively.
- Reinforce to patient the need to avoid lifting, bending, twisting, and sitting for long periods of time.
- Remind patient to change positions frequently.
- Remind patient not to drive while using narcotic pain medications.
- Sexual activity may be resumed as advised by the physician and when comfortable.
- Ensure the patient is aware of return-to-work and activity recommendations.
- Reinforce alternative planning and problem solving for everyday activities (e.g., vacuuming, doing laundry, and performing child care).
- Incision care varies with the type of closure.
- Ensure the patient is aware of postoperative follow-up recommendations.
Postoperative
- Talk to patient about gradually returning to ADLs and lifestyle.
- Patient should begin ambulation within the first 24 hours. Activity will improve pain tolerance and decrease muscle spasms.
- Patient should avoid heavy lifting (anything heavier than a gallon of milk) for the first 4–6 weeks.
- Patient should avoid prolonged sitting or standing for the first 4–6 weeks, including long car trips.
- Patient should begin a walking program that includes progressively longer distances two to three times per day.
- Prescribing an exercise program starting 4–6 weeks post-surgery may lead to a faster decrease in pain and disability than no treatment. High intensity exercise programs
appear to provide a faster decrease in pain and disability than low intensity programs - Patient’s return to work will vary, depending on type of work (sedentary work earlier than heavy labor). Return to work may be a gradual progression to full time.
- Outpatient therapy will be decided on an individual basis and discussed at follow-up surgical visit.
- Patient should be instructed on incision care, dressing removal, bathing, and observation of incision for redness, swelling, or drainage.
- Call surgeon’s office for temperature higher than 100.6° F.
- Patient will gradually be weaned from pain medication.
Common postoperative complications:
- Superficial wound infections
- 0.9%–5% incidence
- Increased risk with age, long-term steroid use, obesity, or diabetes mellitus
- Most superficial infections are caused by S. aureus.
- Mild infections are usually treated with 7–14 days of oral antibiotics.
- Increased motor deficit
- 1%–8% incidence
- Can be transient with nerve root stretching or manipulation.
- Unintended durotomy
- 0.3%–13% incidence
- Generally revealed intraoperatively
- May be repaired with a 4.0 silk or Neuralon, fibrin glue, or muscle plug (may be necessary for poor-quality dura or difficult locations).
- Possible sequelae include a CSF fistula (external CSF leak) or pseudomeningocele.
- A CSF leak generally presents as a wound leak, a collection, or postural headaches.
- In most circumstances, activity is restricted to flat lying position for 24–48 hours. Head of bed is gradually increased.
- In some situations, the physician may elect to have a blood patch placed to plug the tunnel.
- Pseudomeningocele
- 0.7%–2% incidence
- Appears similar radiographically to a spinal epidural abscess.
- If a dural tear is suspected or visualized, the patient is maintained in a flat position for 24–48 hours to minimize dural pressure. Raise the head of the bed slowly (10 degrees every hour) until upright. If the patient complains of positional headache (i.e., headache when upright), then resume flat lying position.
- Some surgeons may place a lumbar drain to decrease dural pressure and allow for dural repair.
- Surgical exploration may be necessary if symptoms do not resolve.
Uncommon complications
- Instability
- Instability is usually found in predisposed patients undergoing decompression without fusion, especially if a significant amount of facet is removed.
- Obtain flexion/extension films to determine amount of movement and need for fusion.
- Direct injury to neural structures
- Deep infections: <1% incidence; this includes discitis at 0.5%, spinal epidural abscess at 0.67%, and osteomyelitis.
- Thrombophlebitis and deep-vein thrombosis with risk of pulmonary embolism: 0.1% incidence.
- Complications of positioning: compression neuropathies, anterior tibial compartment syndrome, pressure on the eye, cervical spine injuries.

