Description and Etiology
Intervertebral disc herniation is also known as herniated nucleus pulposus (HNP). HNP may be asymptomatic despite radiographic evidence of bulging, protrusion, or extruded disc. The etiology may be either nonspecific or attributable to a precipitating event. Even when the patient is symptomatic, surgical intervention often is not required. An HNP may be symptomatic due to a combination of direct nerve root compression, the release of inflammatory chemicals (e.g., matrix metalloproteinases, prostaglandin E2, interleukin- 6, nitric oxide), and hypoxia of the nerve root and basal ganglion (Ireland, 2009). Radicular pain can be accompanied by paresthesias or paresis (i.e., weakness) in the anatomic distribution of the affected nerve root. The patient may complain of low back pain. The back or leg pain may be aggravated by coughing, sneezing, or assuming certain positions.
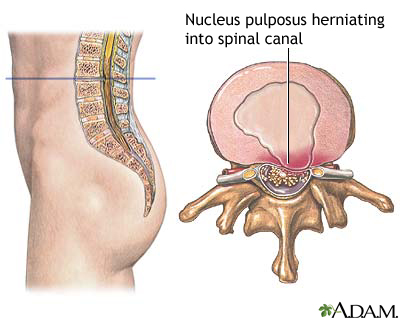
image by : nlm.nih.gov/
Incidence
Most HNPs occur at the L4–L5 or L5–S1 levels. The peak incidence is among people age 35–55. The majority of HNPs occur in a posterolateral direction, compressing the ipsilateral nerve root as it exits the dural sac.
Nursing Assessment, Interventions, and Monitoring
Preoperative
- Describe the surgical procedure to patient and family.
- Informed consent obtained by surgeon.
- Describe the expected outcomes, both postoperative and long term.
- Arrange for required preoperative testing.
- Advise patient to discontinue medications such as herbal products, NSAIDs, anticoagulants, aspirin, warfarin, and clopidogrel bisulfate.
- Encourage patient to anticipate and arrange for perioperative and postoperative care needs.
Perioperative
- Explain to patient where and when to arrive, as well as surgery time.
- Instruct patient as to eating and drinking restrictions.
- Instruct patient about medications to be taken the morning of surgery with a sip of water.
- Remind patient to wear comfortable clothing and to leave jewelry and valuables at home.
- Tell patient to remove dentures, partial plates, eyeglasses, contact lenses, nail polish, and sculptured nails.
Intraoperative
- “Time Out”—right patient, right surgery, right site
- Proper patient positioning
- Table options are surgeon specific.
- If patient is obese, consider using a Jackson table.
- Intraoperative needs anticipation
- Equipment
- Patient-specific needs (e.g., latex allergy)
Postoperative
- Neurological assessment
- Strength and sensation assessment, as compared with preoperative status.
- Special attention to neurological assessment and correlation with the operative intervention.
- Mobility
- Patient should mobilize quickly unless ordered differently due to complication (e.g., CSF leak).
- Instruct and help patient to roll to side and bring legs down while simultaneously rising up with the torso from the bed. This minimizes twisting at the waist.
- Instruct and help patient to rise from a chair using the legs, rather than pushing off with the back.
- Pain control
- The degree of pain varies considerably.
- Intravenous hydromorphone or morphine sulfate may be used as needed until the patient is able to take oral medications.
- Codeine, hydrocodone, or oxycodone, with or without acetaminophen, may be prescribed as needed when the patient is able to take oral medications.
- NSAIDs, as needed, can be very beneficial.
- Neuropathic pain medications (e.g., gabapentin) may be beneficial.
- Antispasmodics may be prescribed if muscle spasms are present.
- Heat may be applied for spasms and muscular tension.
- Ice may be applied for radicular pain for no more than 20 minutes per hour.
- Gentle massage may be used away from the incision.
- Have patient change positions frequently.
- Modest activity may be conducted as tolerated.
- Constipation prevention
- Consider initiating techniques preoperatively.
- Ensure adequate water intake.
- Diet should include adequate fresh fruits, vegetables, and fiber.
- Stool softener (e.g., docusate) may be used two to three times per day.
- Motility agents (e.g., senna) should be used only as needed.
- Urination
- Urinary hesitancy, especially immediately postoperative, is usually transient.
- Assess urinary output, frequency, and volume.
- Assess to be sure there is adequate emptying. Bladder scanning or intermittent bladder catheterization may be necessary to assess for retention or incomplete emptying.
- Discharge planning
- Discharge planning should be initiated preoperatively.
- Reinforce the following: no lifting, bending, or twisting; no sitting for long periods of time.
- Remind patient to change positions frequently.
- Remind patient not to drive while using narcotic pain medications.
- Explain to patient that sexual activity may be resumed 2 weeks after surgery and when it is comfortable.
- Ensure the patient is aware of return-towork and activity recommendations.
- Reinforce alternative planning and problem solving for practical everyday activities (e.g., vacuuming, doing laundry, and performing child care).
- Incision care varies with the type of closure.
- Ensure the patient is aware of postoperative follow-up recommendations.


