Notes

Description
- Appendicitis is inflammation of the appendix.
- When the appendix becomes inflamed or infected, rupture may occur within a matter of hours, leading to peritonitis and sepsis.
Risk Factors
- Obstruction by fecalith or foreign bodies, bacteria or toxins.
- Low-fiber diet
- High intake of refined carbohydrates
Signs and Symptoms/ Assessment
- Pain in the periumbilical area that descends to the right lower quadrant.
- Abdominal pain that is most intense at McBurney’s point
- Rebound tenderness and abdominal rigidity
- Low-grade fever
- Elevated white blood cell count
- Anorexia, nausea, and vomiting
- Client in side-lying position, with abdominal guarding and legs flexed
- Constipation or diarrhea
Diagnostic Evaluation
- Diagnosis is based on a complete physical examination and laboratory and radiologic tests.
- Leukocyte count greater than 10,000/mm 3, neutrophil count greater than 75%; abdominal radiographs, ultrasound studies, and CT scans may reveal right lower quadrant density or localized distention of the bowel.
Primary Nursing Diagnosis
Primary Preoperative Nursing Diagnosis
- Pain (acute) related to inflammation
Primary Postoperative Nursing Diagnosis
- Risk for infection related to the surgical incision
Other Diagnoses that may occur in Nursing Care Plans For Appendicitis
- Imbalanced nutrition: Less than body requirements
- Impaired skin integrity
- Ineffective tissue perfusion: GI
- Risk for deficient fluid volume
- Risk for injury
Medical Management
An appendectomy (surgical removal of the appendix) is the preferred method of management for acute appendicitis if the inflammation is localized. An open appendectomy is completed with a transverse right lower quadrant incision, usually at the McBurney point. A laparoscopic appendectomy may be used in females of childbearing age, those in whom the diagnosis is in question, and for obese patients. If the appendix has ruptured and there is evidence of peritonitis or an abscess, conservative treatment consisting of antibiotics and intravenous (IV) fluids is given 6 to 8 hours prior to an appendectomy. Generally, an appendectomy is performed within 24 to 48 hours after the onset of symptoms under either general or spinal anesthesia. Preoperative management includes IV hydration, antipyretics, antibiotics, and, after definitive diagnosis, analgesics.
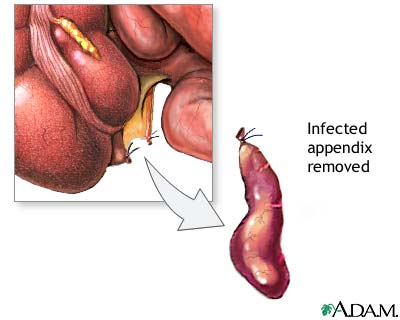
Appendectomy (surgical removal of the appendix)
Complications of Appendectomy
- The major complication is perforation of the appendix, which can lead to peritonitis or an abscess.
- Perforation generally occurs 24 hours after onset of pain, symptoms include fever (37.7°C [100° F] or greater), toxic appearance, and continued pain and tenderness.
Pharmacologic Intervention
- Crystalloid intravenous fluids an isotonic solutions such as normal saline solution or lactated Ringer’s solution 100–500 mL/hr of IV, depending on volume state of the patient, is used to replaces fluids and electrolytes lost through fever and vomiting; replacement continues until urine output is 1 cc/kg of body weight and electrolytes are replaced
- Antibiotics (broad-spectrum antibiotic coverage) to control local and systemic infection and reduces the incidence of postoperative wound infection
- Other Drugs: Analgesics.
Nursing Intervention
Preoperative interventions
- Maintain NPO status.
- Administer fluids intravenously to prevent dehydration.
- Monitor for changes in level of pain.
- Monitor for signs of ruptured appendix and peritonitis
- Position right-side lying or low to semi fowler position to promote comfort.
- Monitor bowel sounds.
- Apply ice packs to abdomen every hour for 20-30 minutes as prescribed.
- Administer antibiotics as prescribed
- Avoid the application of heat in the abdomen.
- Avoid laxatives or enema.
Postoperative interventions
- Monitor temperature for signs of infection.
- Assess incision for signs of infection such as redness, swelling and pain.
- Maintain NPO status until bowel function has returned.
- Advance diet gradually or as tolerated or as prescribed when bowel sound return.
- If ruptured of appendix occurred, expect a Penros drain to be inserted, or the incision maybe left to heal inside out.
- Expect that drainage from the Penros drain maybe profuse for the first 2 hours.
Documentation Guidelines
- Location, intensity, frequency, and duration of pain
- Response to pain medication, ice applications, and position changes
- Patient’s ability to ambulate and tolerate food
- Appearance of abdominal incision (color, temperature, intactness, drainage)
Discharge and Home Healthcare Guidelines
- MEDICATIONS. Be sure the patient understands any pain medication prescribed, including doses, route, action, and side effects. Make certain the patient understands that he or she should avoid operating a motor vehicle or heavy machinery while taking such medication.
- INCISION. Sutures are generally removed in the physician’s office in 5 to 7 days. Explain the need to keep the surgical wound clean and dry. Teach the patient to observe the wound and report to the physician any increased swelling, redness, drainage, odor, or separation of the wound edges. Also instruct the patient to notify the doctor if a fever develops. The patient needs to know these may be symptoms of wound infection. Explain that the patient should avoid heavy lifting and should question the physician about when lifting can be resumed.
- COMPLICATIONS. Instruct the patient that a possible complication of appendicitis is peritonitis. Discuss with the patient symptoms that indicate peritonitis, including sharp abdominal pains, fever, nausea and vomiting, and increased pulse and respiration. The patient must know to seek medical attention immediately should these symptoms occur.
- NUTRITION. Instruct the patient that diet can be advanced to her or his normal food pattern as long as no gastrointestinal distress is experienced.
Sources:
Marilyn Sawyer Sommers, RN, PhD, FAAN , Susan A. Johnson, RN, PhD, Theresa A. Beery, PhD, RN , DISEASES AND DISORDERS A Nursing Therapeutics Manual, 2007 3rd ed
Handbook for Brunner & Suddarth’s, Textbook of Medical-SurgicalNursing, 11th ed
Exam
Nursing Care Plan
Nursing Diagnosis: Acute Pain
May be related to
- Distension of intestinal tissues by inflammation
- Presence of surgical incision
Possibly evidenced by
- Reports of pain
- Facial grimacing, muscle guarding; distraction behaviors
- Expressive behavior (restlessness, moaning, crying, vigilance, irritability, sighing)
- Autonomic responses
Desired Outcomes
- Report pain is relieved/controlled.
- Appear relaxed, able to sleep/rest appropriately.
- Demonstrate use of relaxation skills and diversional activities, as indicates, for individual situation.
Nursing Interventions
- Assess pain, noting location, characteristics, severity (0–10 scale). Investigate and report changes in pain as appropriate.
- Rationale: Useful in monitoring effectiveness of medication, progression of healing. Changes in characteristics of pain may indicate developing abscess or peritonitis, requiring prompt medical evaluation and intervention.
- Provide accurate, honest information to patient and SO.
- Rationale: Being informed about progress of situation provides emotional support, helping to decrease anxiety
- Keep at rest in semi-Fowler’s position.
- Rationale: To lessen the pain. Gravity localizes inflammatory exudate into lower abdomen or pelvis, relieving abdominal tension, which is accentuated by supine position.
- Encourage early ambulation.
- Rationale: Promotes normalization of organ function (stimulates peristalsis and passing of flatus, reducing abdominal discomfort).
- Provide diversional activities
- Rationale: Refocuses attention, promotes relaxation, and may enhance coping abilities.
- Keep NPO and maintain NG suction initially.
- Rationale: Decreases discomfort of early intestinal peristalsis, gastric irritation and vomiting.
- Administer analgesics as indicated.
- Rationale: Relief of pain facilitates cooperation with other therapeutic interventions (ambulation, pulmonary toilet).
- Place ice bag on abdomen periodically during initial 24–48 hr, as appropriate.
- Rationale: Soothes and relieves pain through desensitization of nerve endings. Note: Do not use heat, because it may cause tissue congestion.
- Never apply heat to the right lower abdomen.
- Rationale: This may cause the appendix to rupture.
- Watch closely for possible surgical complications.
- Rationale: Continuing pain and fever may signal an abscess.
Nursing Diagnosis: Risk for Fluid Volume Deficit
Risk factors may include
- Preoperative vomiting, postoperative restrictions (e.g., NPO)
- Hypermetabolic state (e.g., fever, healing process)
- Inflammation of peritoneum with sequestration of fluid
Desired Outcomes
- Hydration (NOC)
- Maintain adequate fluid balance as evidenced by moist mucous membranes, good skin turgor, stable vital signs, and individually adequate urinary output.
Nursing Interventions
- Monitor BP and pulse.
- Rationale: Variations help identify fluctuating intravascular volumes
- Inspect mucous membranes; assess skin turgor and capillary refill.
- Rationale:Indicators of adequacy of peripheral circulation and cellular hydration.
- Monitor I&O; note urine color and concentration, specific gravity.
- Rationale: Decreasing output of concentrated urine with increasing specific gravity suggests dehydration and need for increased fluids.
- Auscultate and document bowel sounds. Note passing of flatus, bowel movement.
- Rationale: Indicators of return of peristalsis, readiness to begin oral intake. Note: This may not occur in the hospital if patient has had a laparoscopic procedure and been discharged in less than 24 hr.
- Provide clear liquids in small amounts when oral intake is resumed, and progress diet as tolerated.
- Rationale: Reduces risk of gastric irritation and vomiting to minimize fluid loss.
- Give frequent mouth care with special attention to protection of the lips.
- Rationale: Dehydration results in drying and painful cracking of the lips and mouth.
- Maintain gastric and intestinal suction, as indicated.
- Rationale: An NG tube may be inserted preoperatively and maintained in immediate postoperative phase to decompress the bowel, promote intestinal rest, prevent vomiting.
- Administer IV fluids and electrolytes.
- Rationale: The peritoneum reacts to irritation and infection by producing large amounts of intestinal fluid, possibly reducing the circulating blood volume, resulting in dehydration and relative electrolyte imbalances.
- Never administer cathartics or enemas.
- Rationale: Cathartics and enemas may rupture the appendix.
- Give the patient nothing by mouth, and administer analgesics judiciously.
- Rationale: This may mask symptoms.
Nursing Diagnosis: Risk for Infection
Risk factors may include
- Inadequate primary defenses; perforation/rupture of the appendix; peritonitis; abscess formation
- Invasive procedures, surgical incision
Desired Outcomes
- Achieve timely wound healing; free of signs of infection/inflammation, purulent drainage, erythema, and fever.
Nursing Priorities
- Prevent complications.
- Promote comfort.
- Provide information about surgical procedure/prognosis, treatment needs, and potential complications.
Discharge Goals
- Complications prevented/minimized.
- Pain alleviated/controlled.
- Surgical procedure/prognosis, therapeutic regimen, and possible complications understood.
- Plan in place to meet needs after discharge.
Nursing Interventions
- Practice and instruct in good handwashing and aseptic wound care. Encourage and provide perineal care.
- Rationale: Reduces risk of spread of bacteria.
- Inspect incision and dressings. Note characteristics of drainage from wound (if inserted), presence of erythema.
- Rationale: Provides for early detection of developing infectious process and monitors resolution of preexisting peritonitis.
- Monitor vital signs. Note onset of fever, chills, diaphoresis, changes in mentation, reports of increasing abdominal pain.
- Rationale: Suggestive of presence of infection or developing sepsis, abscess, peritonitis.
- Obtain drainage specimens if indicated.
- Rationale: Gram’s stain, culture, and sensitivity testing is useful in identifying causative organism and choice of therapy.
- Administer antibiotics as appropriate.
- Rationale: Antibiotics given before appendectomy are primarily for prophylaxis of wound infection and are not continued postoperatively. Therapeutic antibiotics are administered if the appendix is ruptured or abscessed or peritonitis has developed.
- Prepare and assist with incision and drainage (I&D) if indicated.
- Rationale: May be necessary to drain contents of localized abscess.
- Watch closely for possible surgical complications.
- Rationale: Continuing pain and fever may signal an abscess.
Nursing Diagnosis: Deficient Knowledge
May be related to
- Lack of exposure/recall; information misinterpretation
- Unfamiliarity with information resources
Possibly evidenced by
- Questions; request for information; verbalization of problem/concerns
- Statement of misconception
- Inaccurate follow-through of instruction
- Development of preventable complications
Desired Outcomes
- Verbalize understanding of disease process and potential complications.
- Verbalize understanding of therapeutic needs.
- Participate in treatment regimen.
Nursing Interventions
- Identify symptoms requiring medical evaluation (increasing pain; edema or erythema of wound; presence of drainage, fever).
- Rationale: Prompt intervention reduces risk of serious complications (delayed wound healing, peritonitis).
- Review postoperative activity restrictions (heavy lifting, exercise, sex, sports, driving).
- Rationale: Provides information for patient to plan for return to usual routines without untoward incidents.
- Encourage progressive activities as tolerated with periodic rest periods.
- Rationale: Prevents fatigue, promotes healing and feeling of well-being, and facilitates resumption of normal activities.
- Recommend use of mild laxative or stool softeners as necessary and avoidance of enemas.
- Rationale: Assists with return to usual bowel function; prevents undue straining for defecation.
- Discuss care of incision, including dressing changes, bathing restrictions, and return to physician for suture and staple removal.
- Rationale: Understanding promotes cooperation with therapeutic regimen, enhancing healing and recovery process.
- Encourage the patient to cough, breathe deeply, and and turn frequently.
- Rationale: To prevent pulmonary complication
