Notes
Description
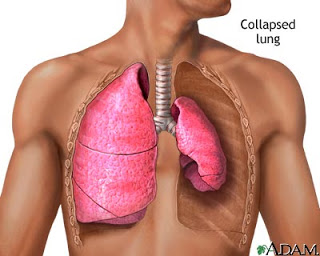
- Pneumothorax is the accumulation of atmospheric air in the pleural space, which results in a rise in intrathoracic pressure and reduced vital capacity.

- The loss of negative intrapleural pressure results in collapse of the lung.
- A spontaneous pneumothorax occurs with the rupture of a bleb.
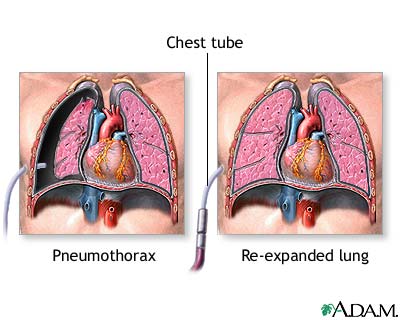
- An open pneumothorax occurs when an opening through the chest wall allows the entrance of positive atmospheric pressure into the pleural space.
- Diagnosis of pneumothorax is made by chest x-ray film.
Causes
The cause of a closed or primary spontaneous penumothorax is the rupture of a bleb (vesicle) on the surface of the visceral pleura. Secondary spontaneous pneumothorax can result from chronic obstructive pulmonary disease (COPD), which is related to hyperinflation or air trapping, or from the effects of cancer, which can result in the weakening of lung tissue or erosion into the pleural space by the tumor. Blunt chest trauma and penetrating chest trauma are the primary causes of traumatic and tension pneumothorax. Other possible causes include therapeutic procedures such as thoracotomy, thoracentesis, and insertion of a central line.
Assessment
- Absent breath sounds on affected side
- Cyanosis
- Decreased chest expansion unilaterally
- Dyspnea
- Hypotension
- Sharp chest pain
- Subcutaneous emphysema as evidenced by crepitus on palpation
- Sucking sound with open chest wound
- Tachycardia
- Tachypnea
- Tracheal deviation to the unaffected side with tension pneumothorax
Complications
- Another collapsed lung in the future
- Shock
Primary Nursing Diagnosis
- Impaired gas exchange related to decreased oxygen diffusion capacity
Diagnostic Evaluation
- Chest x-ray reveals lung collapse with air between chest wall and visceral pleura. Lungs are not filled with air but rather are collapsed.
- Other Tests: Complete blood count, plasma alcohol level, arterial blood gases, rib x-rays, computed tomography (CT) scan.
Medical Management
- The priority is to maintain airway, breathing, and circulation. The most important interventions focus on reinflating the lung by evacuating the pleural air. Patients with a primary spontaneous pneumothorax that is small with minimal symptoms may have spontaneous sealing and lung reexpansion.
- For patients with jeopardized gas exchange, chest tube insertion may be necessary to achieve lung re-expansion.
- Maintain a closed chest drainage system; be sure to tape all connections, and secure the tube carefully at the insertion site with adhesive bandages. Regulate suction according to the chest tube system directions; generally, suction does not exceed 20 to 25 cm H2O negative pressure.
- Monitor a chest tube unit for any kinks or bubbling, which could indicate an air leak, but do not clamp a chest tube without a physician’s order because clamping may lead to tension pneumothorax.
- Stabilize the chest tube so that it does not drag or pull against the patient or against the drainage system. Maintain aseptic technique, changing the chest tube insertion site dressing and monitoring the site for signs and symptoms of infection such as redness, swelling, warmth, and drainage.
- Oxygen therapy and mechanical ventilation are prescribed as needed. Surgical interventions include removing the penetrating object, exploratory thoracotomy if necessary, thoracentesis, and thoracotomy for patients with two or more episodes of spontaneous pneumothorax or patients with pneumothorax that does not resolve within 1 week.
Pharmacologic Highlights
No routine pharmacologic measures will treat pneumothorax, but the patient may need antibiotics, local anesthesia agents for procedures, and analgesics, depending on the extent and nature of the injury. Analgesia is administered for pain once the patient’s pulmonary status has stabilized.
Nursing Interventions
- Apply a dressing over an open chest wound.
- Administer oxygen as prescribed.
- Position the client in high fowler’s position.
- Prepare for chest tube placement until the lung has expanded fully.
- Monitor chest tube drainage system.
- Monitor for subcutaneous emphysema.
Documentation Guidelines
- Physical findings: Breath sounds, vital signs, level of consciousness, urinary output, skin temperature, amount and color of chest tube drainage, dyspnea, cyanosis, nasal flaring, altered chest expansion, tracheal deviation, absence of breath sounds
- Response to pain: Location, description, duration, response to interventions
- Response to treatment: Chest tube insertion—type and amount of drainage, presence of air leak, presence or absence of crepitus, amount of suction, presence of clots, response to fluid resuscitation; response to surgical management
- Complications: Infection (fever, wound drainage); inadequate gas exchange (restlessness, dropping SaO2); tension pneumothorax
Discharge and Home Healthcare Guidelines
- Review all follow-up appointments, which often involve chest x-rays, arterial blood gas analysis, and a physical exam. If the injury was alcohol-related, explore the patient’s drinking pattern.
- Refer for counseling, if necessary. Teach the patient when to notify the physician of complications (infection, an unhealed wound, and anxiety) and to report any sudden chest pain or difficulty breathing.
Exam
Nursing Care Plan
Pneumothorax & Hemothorax Nursing Care Plan
Nursing Diagnosis
- Breathing Pattern, ineffective
May be related to
- Decreased lung expansion (air/fluid accumulation)
- Musculoskeletal impairment
- Pain/anxiety
- Inflammatory process
Possibly evidenced by
- Dyspnea, tachypnea
- Changes in depth/equality of respirations; altered chest excursion
- Use of accessory muscles, nasal flaring
- Cyanosis, abnormal ABGs
Desired Outcomes
- Establish a normal/effective respiratory pattern with ABGs within patient’s normal range.
- Be free of cyanosis and other signs/symptoms of hypoxia.
Nursing Interventions
- Determine etiology and precipitating factors (spontaneous collapse, trauma, malignancy, infection, complication of mechanical ventilation).
- Rationale: Understanding the cause of lung collapse is necessary for proper chest tube placement and choice of other therapeutic measures.
- Check out respiratory function, noting rapid or shallow respirations, dyspnea, reports of “air hunger,” development of cyanosis, changes in vital signs.
- Rationale: Respiratory distress and changes in vital signs may occur as a result of physiological stress and pain or may indicate development of shock due to hypoxia or hemorrhage.
- Observe for synchronous respiratory pattern when using mechanical ventilator. Note changes in airway pressures.
- Rationale: Difficulty breathing “with” ventilator and increasing airway pressures suggests worsening of condition or development of complications (spontaneous rupture of a bleb creating a new pneumo -thorax).
- Auscultate breath sounds.
- Rationale: Breath sounds may be diminished or absent in a lobe, lung segment, or entire lung field (unilateral). Atelectatic area will have no breath sounds, and partially collapsed areas have decreased sounds. Regularly scheduled evaluation also helps determine areas of good air exchange and provides a baseline to evaluate resolution of pneumothorax.
- Note chest excursion and position of trachea.
- Rationale: Chest excursion is unequal until lung re-expands. Trachea deviates away from affected side with tension pneumothorax.
- Evaluate fremitus.
- Rationale: Voice and tactile fremitus (vibration) is reduced in fluid-filled or consolidated tissue.
- Assist patient with splinting painful area when coughing, deep breathing.
- Rationale: Supporting chest and abdominal muscles makes coughing more effective and less traumatic.
- Maintain position of comfort, usually with head of bed elevated. Turn to affected side. Encourage patient to sit up as much as possible.
- Rationale: Promotes maximal inspiration; enhances lung expansion and ventilation in unaffected side.
- Maintain a calm attitude, assisting patient to “take control” by using slower and deeper respirations.
- Rationale: Assists patient to deal with the physiological effects of hypoxia, which may be manifested as anxiety or fear.
- Once chest tube is inserted:
- Rationale: Maintains prescribed intrapleural negativity, which promotes optimum lung expansion and fluid drainage. Note: Dry- seal setups are also used with an automatic control valve (AVC), which provides a one-way valve seal similar to that achieved with the water-seal system.
- Check suction control chamber for correct amount of suction (determined by water level, wall or table regulator at correct setting;
- Rationale: Water in a sealed chamber serves as a barrier that prevents atmospheric air from entering the pleural space should the suction source be disconnected and aids in evaluating whether the chest drainage system is functioning appropriately. Note: Underfilling the water-seal chamber leaves it exposed to air, putting patient at risk for pneumothorax or tension pneumothorax. Overfilling (a more common mistake) prevents air from easily exiting the pleural space, thus preventing resolution of pneumothorax or tension pneumothorax.
Monitor fluid level in water-seal chamber; maintain at prescribed level;
- Observe water-seal chamber bubbling;
- Rationale: Bubbling during expiration reflects venting of pneumothorax (desired action). Bubbling usually decreases as the lung expands or may occur only during expiration or coughing as the pleural space diminishes. Absence of bubbling may indicate complete lung re-expansion (normal) or represent complications such as obstruction in the tube.
- Observe for abnormal and continuous water-seal chamber bubbling;
- Rationale: With suction applied, this indicates a persistent air leak that may be from a large pneumothorax at the chest insertion site (patient-centered) or chest drainage unit (system-centered).
- Know the location of air leak (patient- or system-centered) by clamping thoracic catheter just distal to exit from chest;
- Rationale: If bubbling stops when catheter is clamped at insertion site, leak is patient- centered (at insertion site or within the patient).
- Place petrolatum gauze and other appropriate material around the insertion as indicated.
- Rationale: Usually corrects insertion site air leak.
- Clamp tubing in stepwise fashion downward toward drainage unit if air leak continues;
- Rationale: Isolates location of a system-centered air leak.Note: Information indicates that clamping for a suspected leak may be the only time that chest tube should be clamped.
- Seal drainage tubing connection sites securely with lengthwise tape or bands according to established policy;
- Rationale: Prevents and corrects air leaks at connector sites.
- Monitor water-seal chamber “tidaling.” Note whether change is transient or permanent;
- Rationale: The water-seal chamber serves as an intrapleural manometer (gauges intrapleural pressure); therefore, fluctuation (tidaling) reflects pressure differences between inspiration and expiration. Tidaling of 2–6 cm during inspiration is normal and may increase briefly during coughing episodes. Continuation of excessive tidal fluctuations may indicate existence of airway obstruction or presence of a large pneumothorax.
- Position drainage system tubing for optimal function like shorten tubing or coil extra tubing on bed, making sure tubing is not kinked or hanging below entrance to drainage container. Drain accumulated fluid as necessary;
- Rationale: Improper position, kinking, or accumulation of clots or fluid in the tubing changes the desired negative pressure and impedes air or fluid evacuation. Note: If a dependent loop in the drainage tube cannot be avoided, lifting and draining it every 15 min will maintain adequate drainage in the presence of a hemothorax.
- Assess amount of chest tube drainage, noting whether tube is warm and full of blood and bloody fluid level in water-seal bottle is rising;
- Rationale: Useful in evaluating resolution of pneumothorax and development of hemorrhage requiring prompt intervention. Note: Some drainage systems are equipped with an autotransfusion device, which allows for salvage of shed blood.
- Evaluate need for tube stripping (“milking”);
- Rationale: Although routine stripping is not recommended, it may be necessary occasionally to maintain drainage in the presence of fresh bleeding, large blood clots or purulent exudate (empyema).
- Strip tubes carefully per protocol, in a manner that minimizes excess negative pressure.
- Rationale: Stripping is usually uncomfortable for patient because of the change in intrathoracic pressure, which may induce coughing or chest discomfort. Vigorous stripping can create very high intrathoracic suction pressure, which can be injurious (invagination of tissue into catheter eyelets, collapse of tissues around the catheter, and bleeding from rupture of small blood vessels).
If thoracic catheter is disconnected or dislodged:
- Observe for signs of respiratory distress. If possible, reconnect thoracic catheter to tubing or suction, using clean technique. If the catheter is dislodged from the chest, cover insertion site immediately with petrolatum dressing and apply firm pressure. Notify physician at once.
- Rationale: Pneumothorax may recur, requiring prompt intervention to prevent fatal pulmonary and circulatory impairment.
After thoracic catheter is removed:
- Cover insertion site with sterile occlusive dressing. Observe for signs and symptoms that may indicate recurrence of pneumothorax (shortness of breath, reports of pain. Inspect insertion site, note character of drainage).
- Rationale: Early detection of a developing complication is essential (recurrence of pneumothorax, presence of infection).
- Review serial chest x-rays.
- Rationale: Monitors progress of resolving hemothorax or pneumothorax and re-expansion of lung. Can identify malposition of endotracheal tube (ET) affecting lung re-expansion.
- Monitor and graph serial ABGs and pulse oximetry. Review vital capacity and tidal volume measurements.
- Rationale: Assesses status of gas exchange and ventilation, need for continuation or alterations in therapy.
- Administer supplemental oxygen via cannula, mask, or mechanical ventilation as indicated.
- Rationale: Aids in reducing work of breathing; promotes relief of respiratory distress and cyanosis associated with hypoxemia.
Nursing Diagnosis
- Risk for Trauma
- Risk for Suffocation
Risk factors may include
- Concurrent disease/injury process
- Dependence on external device (chest drainage system)
- Lack of safety education/precautions
Desired Outcomes
- Recognize need for/seek assistance to prevent complications.
- Correct/avoid environmental and physical hazards.
Nursing Interventions
- Explain with patient purpose and function of chest drainage unit, taking note of safety features.
- Rationale: Information on how system works provides reassurance, reducing patient anxiety.
- Advise patient to avoid lying and pulling on tubing.
- Rationale: Reduces risk of obstructing drainage and inadvertently disconnecting tubing.
- Identify changes or situations that should be reported to caregivers such as change in sound of bubbling, sudden “air hunger” and chest pain, disconnection of equipment.
- Rationale: Timely intervention may prevent serious complications.
- Anchor thoracic catheter to chest wall and provide extra length of tubing before turning or moving patient;
- Rationale: Prevents thoracic catheter dislodgment or tubing disconnection and reduces pain and discomfort associated with pulling or jarring of tubing.
- Secure tubing connection sites;
- Rationale: Prevents tubing disconnection.
- Pad banding sites with gauze or tape.
- Rationale: Protects skin from irritation and pressure.
- Secure drainage unit to patient’s bed, stand or cart placed in low-traffic area.
- Rationale: Maintains upright position and reduces risk of accidental tipping and breaking of unit.
- Implement safe transportation if patient is sent off unit for diagnostic purposes. Before transporting: check water-seal chamber for correct fluid level, presence or absence of bubbling; presence, degree and timing of tidaling. Ascertain whether or not chest tube can be clamped or disconnected from suction source.
- Rationale: Promotes continuation of optimal evacuation of fluid or air during transport. If patient is draining large amounts of chest fluid or air, tube should not be clamped or suction interrupted because of risk of reaccumulation of fluid or air, compromising respiratory status.
- Observe thoracic insertion site, noting condition of skin, presence and characteristics of drainage from around the catheter. Change or reapply sterile occlusive dressing as needed.
- Rationale: Provides for early recognition and treatment of developing skin or tissue erosion or infection.
- Observe for signs of respiratory distress if thoracic catheter is disconnected or dislodged.
- Rationale: Pneumothorax may recur or worsen, compromising respiratory function and requiring emergency intervention.
Nursing Diagnosis
- Knowledge, deficient [Learning Need] regarding condition, treatment regimen, self-care, and discharge needs
May be related to
- Lack of exposure to information
Possibly evidenced by
- Expressions of concern, request for information
- Recurrence of problem
Desired Outcomes
- Verbalize understanding of cause of problem (when known).
- Identify signs/symptoms requiring medical follow-up.
- Follow therapeutic regimen and demonstrate lifestyle changes if necessary to prevent recurrence.
Nursing Interventions
- Ascertain pathology of individual problem.
- Rationale: Information reduces fear of unknown. Provides knowledge base for understanding underlying dynamics of condition and significance of therapeutic interventions.
- Determine likelihood for recurrence and long-term complications.
- Rationale: Certain underlying lung diseases such as severe COPD and malignancies may increase incidence of recurrence. In otherwise healthy patients who suffered a spontaneous pneumothorax, incidence of recurrence is 10%–50%. Those who have a second spontaneous episode are at high risk for a third incident (60%).
- Reassess signs and symptoms requiring immediate medical evaluation such as sudden chest pain, dyspnea or air hunger, progressive respiratory distress.
- Rationale: Recurrence of pneumothorax or hemothorax requires medical intervention to prevent or reduce potential complications.
- Review significance of good health practices (adequate nutrition, rest, exercise).
- Rationale: Maintenance of general well-being promotes healing and may prevent or limit recurrences.


