Definition
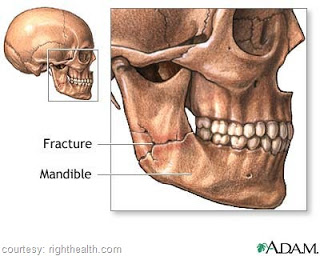
The correction of a fractured lower jaw by either the closed or open method.
Discussion
- Repair of fractured mandible, like the majority of facial fractures, may require a multidisciplinary approach, including dental, nasal, and orthopedic surgery, with appropriate instrumentation.
- Numerous presentations occur and all must be reduced and stabilized as soon as possible after the injury.
- The reduction, like any other fracture, may be corrected by either the open or closed method. When the fracture is anterior (teeth are on either side of the fracture), intermaxillary fixation may be all that is necessary. For fractures occurring posterior to the teeth, intermaxillary fixation and open reduction is usually required.
- Two methods:
- Closed method: Application of arch bars, used by themselves or applied in conjunction with an open reduction procedure.
- Open method: Incision into the mandible; reduction of the fracture with jaw wiring and application of arch bars
Positioning
- Supine (for both open and closed); arms may be tucked in at the sides; head positioned on a headrest.
Packs/Drapes
- Closed reduction procedure is considered “clean”, not strerile. Only the instrument table or mayo tray must be draped with sterile drape sheets, and only gloves are required. A towel is used to cover the eyes and sheet to cover the patient.
- Open reduction a sterile set up is required; head drape with a basic pack and split sheet.
Instrumentation
Closed reduction and application of intermaxillary wiring.
- Minor orthopedic tray
- Plastic tray
- Power drill
- Arch bars
- Wire cutter
Open reduction
- Minor orthopedic tray
- Power drill
- Plastic tray
Supplies/ Equipment
Closed reduction
- Head rest
- Suction
- Power source for drill
Open reduction
- Basin set
- Power source drill
- Stainless teel wire
- Blades
- Needle counter
- Solutions
- Sutures
- Drain
- Nerve stimulator
Procedure Overview
Closed reduction
- An arch bar, available in precut lengths, is bent to fit the contour of the patient’s maxillary and mandibular arches.
- The bars are attached by passing short lengths of 25 to 26 gauge stainless steel wires between the teeth and around the bar.
- Additional wires or small elastic bands are looped around the bars to occlude the jaw.
Open reduction
- Access is gained to the fractures site by sharp dissection through the skin and muscle layers of the lower jaw (mandible).
- A small rake retractor is used to retract the wound edges, and two small bone-holding clamps are used to stabilize the fracture site.
- Using a small drill point, mounted on a power drill, small holes are made through each of the bone fragments, and the wires are passed through the holes to maintain alignment.
- The wire is grasped with a blunt needle holder and twisted; the ends are cut.
- The periosteum and muscle layers are closed with interrupted absorbable suture, and the skin is closed.
- A small drain may be placed in the wound, and arch bars may be applied prior to or following the open reduction.
Perioperative Nusring Considerations
- It is crucial that a wire cutter be sent with the patient to the P.A.C.U in the event the jaw must be freed in an emergency.
- If arch bars or other intermaxillary wiring devices are applied first, a separate set-up is required for the open reduction.
- The table may be turned to facilitate access; do not allow preparation solution to pool in or around the eyes or ears.
- A method for patient communication such as wipe-off writing tablet and call bell, must be available since verbal communication will not be possible as long as the jaw remains wired.

