Description
Myxedema coma is a life-threatening condition in which patients with underlying throid dysfunction exhibit exaggerated manifestations of hypothyroidism. Precipitating factors may include (but are limited to) infection, trauma, surgery, heart failure, stroke, or central nervous system depressants. Hypothyroidism depresses metabolic rate, thus seriously affecting all body system.
Signs And Symptoms
- Hypothermia
- Hypoventilation
- Decreased mental function
- Fatigue
- Activity intolerance
- Hyporeflexia
- Cardiac or respiratory failure
Physical Examination
Vital Signs
- BP: hypotension or hypertension
- HR: bradycardia
- RR: bradypnea
- Temperature: hypothermic <95° F (35° C)
Skin
- Coarse and dry
- Possibly carotene color
- Preorbital and facial edema
Neurologic
- Obtunded, coma or seizures
- Delayed reflexes
Gastrointestinal
- Decreased bowel sounds
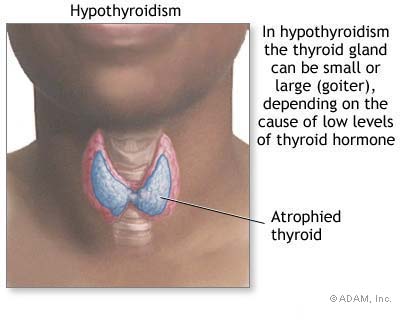
Endocrine
- Thyroid maybe nonpalpable, enlarged, or nodular
Acute Care Patient Management
NURSING DIAGNOSIS: Decreased cardiac output related to bradycardia and decreased stroke volume.
Outcome Criteria
- Patient alert and oriented
- BP 90 to 120 mm Hg
- Mean arterial pressure 70 to 105 mm Hg
- HR 60 to 100 beats/min
- Urine output 30 ml/hr
- Peripheral pulses palpable
Patient Monitoring
- Continuously monitor ECG for dysrhythmias or profound bradycardia that can adversely affect cardiac output.
- Continuously monitor pulmonary artery pressure, central venous pressure (if available) and blood pressure.
- Monitor fluid volume status; measure urine output hourly and determine fluid balance every 8 hours.
Patient Assessment
- Assess cardiovascular status: note quality of peripheral pulses and capillary refill.
- Observe for increase jugular vein distention and pulsus paradoxus, which may indicate pericardial effusion.
Diagnostic Assessment
- Review thyroid studies as available.
- Thyroid stimulating hormone should decline within 24 hours of therapy and should normalize after 7 days of therapy.
Patient Management
- Administer intravenous fluids as ordered to maintain BP >90 mm Hg; carefully monitor for fluid overload and development of heart failure.
- Vasopressor agents may be used if hypotension is refractory to volume administration and if thyroid replacement has not had time to act. Carefully monitor the patient for lethal dysrhythmias.

