Description
Upper gastrointestinal bleeding is characterized by the sudden onset of bleeding from the GI tract at a site (or sites) proximal to the ligament of Treitz. Most upper GI bleeds are a direct result of peptic ulcer erosion, stress related- mucosal disease, that may evidence as superficial erosive gastric lesion to frank ulcerations, erosive gastritis (secondary to use or abuse of NSAIDs, oral corticosteroids, or alcohol) or esophageal varices (secondary to hepatic failure). In addition to these, Mallory-Weiss tears can cause gastroesophageal bleeding as a result of severe retching and vomiting, but the bleeding tends to be less severe than in other types. Hospitalized critically ill patients are at heightened risk for stress related mucosal disease, particularly if they are intubated and mechanically ventilated and/or evidencing coagulopathies.
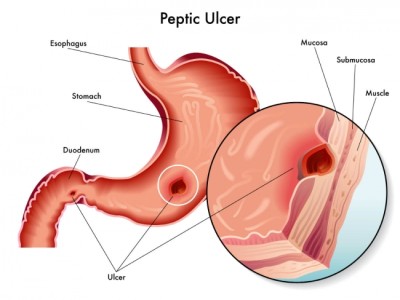
image credit : http://www.practicalpainmanagement.com/
Signs and Symptoms
- Melena and hematemesis
- Pain
- Hypovolemic shock
Physical Examination
Vital signs
- BP < 90 mm Hg
- HR > 100 beats/min
- RR: tachycardia
- Temperature: maybe elevated
Other
- Hematemesis
- Melena
- Bloody stool with fetid odor
- Coffee ground gastric aspirate
Skin
- Pale, diaphoretic
- Cool, clammy
- Jaundice
Cardiovascular
- Weak, thready pulse
- Capillary refill > 3 sec
Abdominal
- Maybe tender with guarding
- Bowel sounds hyperactive or absent
Acute Care Patient Management
Nursing Diagnosis: Deficient fluid volume related to blood loss from hemorrhage.
Outcome Criteria
- Patient alert and oriented
- Skin, pink, warm, and dry
- CVP 2 to 6 mm Hg
- PAS 15 TO 30 mm Hg
- PAD 5 to 15 mm Hg
- BP 90 to 120 mm Hg
- MAP 70 to 105 mm Hg
- HR 60 to 100 beats/min
- Urine output 30 ml/hr
Patient Monitoring
- Obtain pulmonary artery pressure, central venous pressure and blood pressure every 15 minutes during acute episodes to evaluate fluid needs and the patient’s response to therapy.
- Monitor fluid volume status. Measure intake and output hourly to evaluate renal perfusion.
- Measure blood loss if possible.
- Continuously monitor ECG for dysrythmias and myocardial ischemia.
Patient Assessment
- Assess patient for increases restlessness, apprehension or altered consciousness, which may indicate decreased cerebral perfusion.
- Assess hydration status.
- Be alert for recurrence of bleedings.
Diagnostic Assessment
- Review Hgb and Hct levels to determine the effectiveness of treatment or worsening of the patient’s condition.
- Review clotting factors and serum calcium levels if multiple transfusions have been give.
- Review serial BUN levels.
- Review serial ABGs to evaluate oxygenation and acid-base status.
- Review the result of endoscopic evaluation.
Patient Management
- Maintain a patent airway. Administer supplemental oxygen as ordered.
- Administer colloids as ordered to restore intravascular volume.
- Type and crossmatch for anticipated blood products.
- Evacuate stomach contents with nasogastric tube and initiate lavages with room temperature water or saline to clear blood clots from the stomach.
- Continue to monitor the patient closely once stabilized.
- Vitamin K or fresh-frozen plasma (FFP) may be ordered to correct coagulation deficiencies.
- Explain all procedures and tests to the patient to help alleviate anxiety and decreased tissue oxygen demands.


