Definition
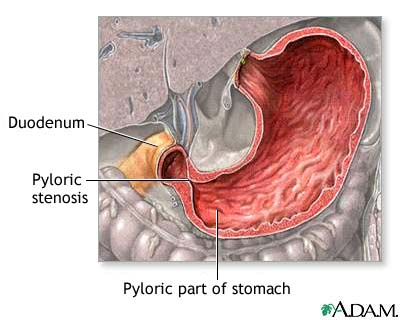
The incision and suturing of the muscles of the pylorus to treat congenital hypertrophy of the pyloric sphincter (pyloric stenosis) that can cause pyloric and/ or gastric obstruction.
Discussion
- The Ramsted-Fredet pyloromyotomy is the procedure of choice to correct this defect surgically.
- Signs and symptoms of high gastrointestinal obstruction usually appear at around 2 to 6 weeks of age, with first symptom being projectile vomiting that is free of bile.
- As a precautionary measure, the stomach is emptied via a nasogastric tube prior to induction of anesthesia, and the nasogastric tube is then removed to prevent gastric contents from accumulating around the tube during the procedure.
Positioning
- Supine, with arms restrained at the side.
Packs/ Drapes
- Pediatric transverse Lap sheet or basic pack and sheet with small fenestration.
Instrumentation
- Pediatric laparotomy tray
- Pyloric spreaders
Supplies/ Equipment
- Thermal blanket with control unit
- Thermal sheets, head covering
- Basin set
- Handheld cautery
- Blades
- Needle counter
- Dissector sponges
- Solutions
- Sutures
Procedure Overview
- The abdomen is opened through a right subcostal transverse incision, splitting the rectus muscle vertically and excising the peritoneum.
- The pylorus is delivered into the wound and rotated to expose the anterior superior border of the mass.
- Using a pyloric spreader, all remaining circular muscle fibers are separated to the level of the submucosa.
- Any lacerations of the gastric or duodenal mucosa are immediately repaired.
- After hemostasis is achieved, the peritoneum and posterior rectus sheath are closed with a continuous absorbable suture.
- The anterior rectus sheath is closed with absorbable suture and the skin is closed using a subcuticular technique.
- Steri-strips are applied with an abdominal dressing.
Perioperative Nursing Considerations
- Maintain aseptic technique during the procedure.
- If tape is being used during positioning, do not allow tape directly contact the skin.
- Do not begin skin preparation without specific instruction from the surgeon.