Description
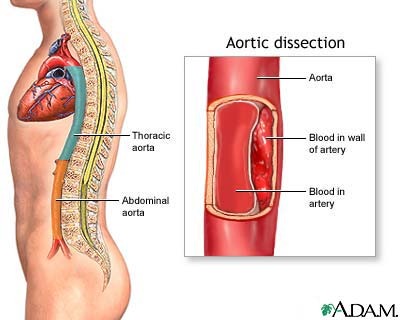
Aortic dissection involves a tear in the medial layer of the aortic wall, causing blood to extravasate into the media and thus compromising blood flow to the brain, heart, and other organs. Usually the causative factor is an underlying disease of the media. Dissection can be classified by the sites involved:
- DeBakey type I – ascending aorta beyond arch.
- DeBakey type II – ascending aorta.
- DeBakey type III – descending aorta.
Demographic risk factors include being male, African American, and in the fifth to seventh decade of life. Medical risk factors include hypertension, aortic valve disease, coarctation of the aorta, Marfan’s syndrome, recent deceleration injury, cocaine use, and complications from invasive procedures such as angiography or intraaortic balloon.
Signs and Symptoms
- Abrupt, severe, tearing pain that may be localized in the anterior chest, intrascapular, abdominal, or lumbar area. The pain is usually nonprogressive and most intense at its onset.
Physical Examination
Appearance
- Anxiety
- Paleness
- Restless
Vital signs
- Increased blood pressure may be > 150 mm Hg
- Decreased blood pressure, if hypovolemic (aortic rupture) or cardiac tamponade develops.
Neurologic
- Intermittent lightheadedness
- Level of consciousness changes
- Weakness
- CVA symptoms
Cardiovascular
- Diastolic murmur (aortic insufficiency) may be present
- Pulse deficits and BP differences between right and left or upper and lower limbs may be noted.
Acute Care Management
Nursing Diagnosis: Ineffective tissue perfusion related to compromised arterial blood flow secondary to blood extravasation via aortic dissection.
Outcome Criteria
- Patient alert and oriented
- Skin war and dry
- BP 80 to 100 mm Hg or as low as can possibly maintain systemic perfusion.
- Urine output 30 mL/hr or 0.5 to 1 ml/kg/hr
- Pulses strong and equal bilaterally
- Capillary refill <3 sec in all extremities
- Pupils equal and nonreactive
- Motor strength strong and equal bilaterally
Nursing Interventions
Patient Monitoring
- Continuously monitor arterial BP during acute phase to evaluate the patient’s response to therapy.
- Monitor hourly urine output because a drop in output may indicate renal artery dissection or a decrease in arterial blood flow.
- Continuously monitor ECG for dysrythmia formation, ST segment or T-wave changes, suggesting coronary sequelae or a decrease in arterial blood flow.
Patient Assessment
- Assess neurologic status to evaluate the course of dissection. Confusion or changes in sensation and motor strength may indicate compromised cerebral blood flow (CBF).
- Auscultate for changes in heart sound and signs and symptoms of heart failure, which may indicate that the dissection involves the aortic valve.
- Compare BP and pulses in both arms and legs to determine differences.
Diagnostic Assessment
- Review serial BUN and creatinine levels to evaluate renal function.
- Review cardiac enzymes because a dissection involving coronary arteries may result in Myocardial Infarction.
- Review the ECG for patterns of ischemia, injury, and infarction.
- Review results of radiology test such as CT scan, MRI, and aotogram.
Patient Management
- Administer oxygen therapy as ordered.
- Keep the patient on bed rest to prevent further dissection
- Nitroprusside may be ordered to lower BP.
- A ?-adrenergic blocking agent such as atenolol, esmolol, or propranolol may be ordered to reduce stress on the aortic wall.
- Anticipate surgical intervention.

