Notes
Definition
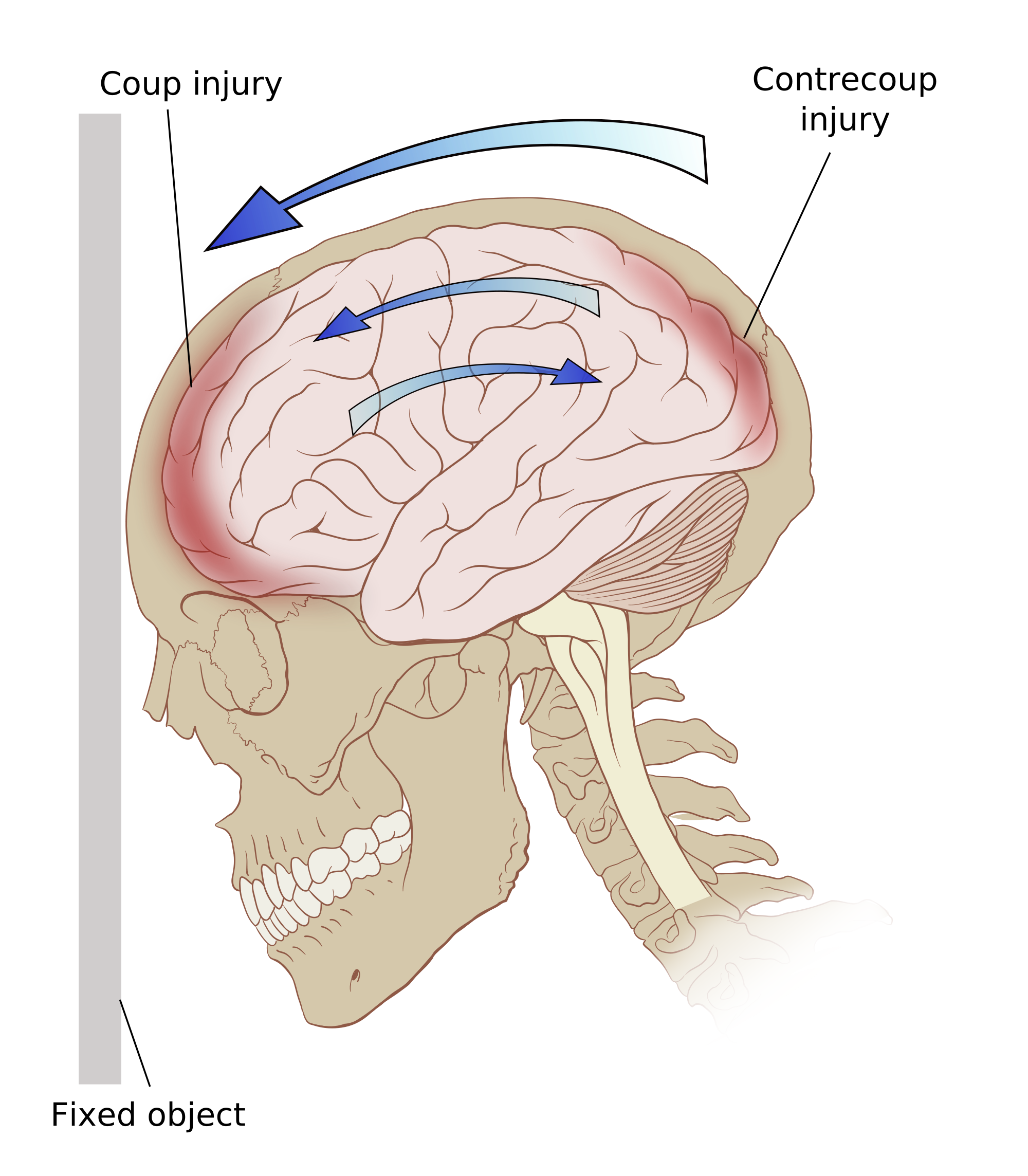
- Also known as head injury.
- Is the disruption of normal brain function due to trauma-related injury resulting in compromised neurologic function resulting in focal or diffuse symptoms.
- Motor vehicle accidents are the most common etiology of injury.
Etiology And Pathophysiology
Types of Traumatic Brain Injury
- Concussion – transient interruption in brain activity; no constructural injury noted on radiographics.
- Cerebral contusion – bruising of brain with associated swelling.
- Intracerebral hematoma – bleeding into the brain tissue commonly associated with edema.
- Epidural hematoma – blood between the inner table of the skull and dura.
- Subdural hematoma – blood between the dura and arachnoid caused by bleeding commonly associated with additional brain injury.
- Diffuse axonal injury – axonal tears within the white matter of the brain.
Assessment
- Disturbance in level of consciousness from slightly drowsy to unconscious.
- Headache, vertigo, agitation, and restlessness.
- Cerebrospinal fluid leakage at ears and nose, which may indicate skull fracture.
- Contusions about eyes and ears indicating skull fractures.
- Irregular respirations
- Cognitive deficit
- Pupillary abnormality
- Sudden onset of neurologic deficits
- Otorrhea indicating posterior fossa skull fracture
- Rhinorrhea indicating anterior fossa skul fracture.
Nursing Diagnosis
- Risk for injury related to complications of head injury.
- Acute pain related to altered brain or skull tissue.
Diagnostic Evaluation
- CT identifies and localizes lesions, cerebral edema, and bleeding.
- Skull and cervical spine X-ray identify fracture and displacement.
- Complete blood count, coagulation profile, electrolyte levels, serum osmolarity, arterial blood gases, and other laboratory tests monitor for complications.
- Neuropsychological test during rehabilitation phase determine cognitive deficits.
Nursing Interventions
- Maintain ICP monitoring, as indicated, and report abnormalities.
- Maintain patent airway; assist with intubation and ventilatory assistance is needed.
- Turn the patient every 2 hours and encourage coughing and deep breathing.
- Apply firm pressure over puncture site for subdural trap, and observe for drainage and dressing.
- Suction the patient as needed.
- Institute measures to prevent increased ICP or other neurovascular compromise.
- Feed the patient as soon as possible after a head injury and administer histamine-2 blockers to prevent gastric ulceration and hemorrhage from gastric acid hypersecretion.
- If the patient is unable to swallow, provide enteral feedings after bowel sounds have returned.
- Elevate the head of the bed after feedings, and check residuals to prevent aspiration.
- Monitor respiratory rate, depth, and pattern of respirations.
Complications
- Infections
- Increased intracranial pressure
- Posttraumatic seizure disorder
- Permanent neurologic deficits
- Persistent sympathetic storming
- SIADH
- Death
Exam
[mtouchquiz 564]

