Notes

Description
- Is a sudden decline in renal function, usually marked by increased concentrations of blood urea nitrogen (BUN; azotemia) and creatinine; oliguria (less than 500 ml of urine in 24 hours); hyperkalemia; and sodium retention.
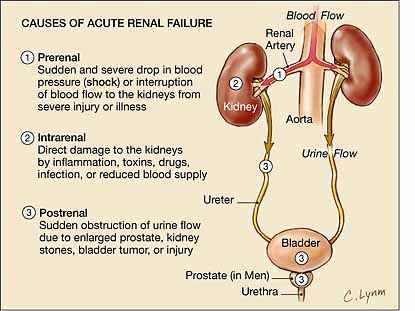
- Acute renal failure are classified into following:
-
- Prerenal failure – results from conditions that interrupt the renal blood supply; thereby reducing renal perfusion (hypovolemia, shock, hemorrhage, burns impaired cardiac output, diuretic therapy).
- Postrenal failure – results from obstruction of urine flow.
- Intrarenal failure – results from injury to the kidneys themselves (ischemia, toxins, immunologic processes, systemic and vascular disorders).
- The disease progresses through three clinically distinct phase which is oliguric-anuric, diuretic, and recovery, distinguished primarily by changes in urine volume and BUN and creatinine levels.
- Complication of ARF include dysrhythmias, increased susceptibility to infection, electrolyte abnormalities, GI bleeding due to stress ulcers, and multiple organ failure. Untreated ARF can also progress to chronic renal failure, end-stage renal disease, and death from uremia or related causes.
Pathophysiology
Assessment:

- Oliguric-anuric phase: urine volume less than 400 ml per 24 hours; increased in serum creatinine, urea, uric acid, organic acids, potassium, and magnesium; lasts 3 to 5 days in infants and children, 10 to 14 days in adolescents and adults.
- Diuretic phase: begins when urine output exceeds 500 ml per 24 hours, end when BUN and creatinine levels stop rising; length is availabe.
- Recovery phase: asymptomatic; last several months to 1 year; some scar tissue may remain.
- In prerenal disease: decreased tissue turgor, dryness of mucous membranes, weight loss, flat neck veins, hypotension, tachycardia.
- In postrenal disease: difficulty in voiding, changes in urine flow.
- In Intrarenal disease: presentation varies; usually have edema, may have fever, skin rash.
- Nausea, vomiting, diarrhea, and lethargy may also occur.
Diagnostic Evaluation:
- Urinalysis shows proteinuria, hematuria, casts. Urine chemistry distinguishes various forms of ARF(prerenal, postrenal, intrarenal).
- Serum creatinine and BUN levels are elevated; arterial blood gas (ABG) levels, serum electrolytes may be abnormal.
- Renal ultrasonography estimates renal size and rules out treatable obstructive uropathy.
Primary Nursing Diagnosis
- Fluid volume deficit related to excessive urinary output,vomiting,hemorrhage
Other Diagnoses that may occur in Nursing Care Plans For Acute Renal Failure
- Ineffective tissue perfusion (renal)
- Excess fluid volume
- Risk for infection
Therapeutic and Pharmacologic Interventions:
- Surgical relief of obstruction may be necessary.
- Correction of underlying fluid excesses or deficits.
- Correction and control of biochemical imbalances.
- Restoration and maintenance of blood pressure through I.V. fluids and vasopressors.
- Maintenance of adequate nutrition: Low protein diet with supplemental amino acids and vitamins.
- Initiation of hemodialysis, peritoneal dialysis, or continuous renal replacement therapy for patients with progressive azotemia and other life-threatening complications.
Nursing Interventions:
- Monitor 24-hour urine volume to follow clinical course of the disease.
- Monitor BUN, creatinine, and electrolyte.
- Monitor ABG levels as necessary to evaluate acid-base balance.
- Weigh the patient to provide an index of fluid balance.
- Measure blood pressure at various times during the day with patients in supine, sitting, and standing positions.
- Adjust fluid intake to avoid volume overload and dehydration.
- Watch for cardiac dysrhythmias and heart failure from hyperkalemia, electrolyte imbalance, or fluid overload. Have resuscitation equipment available in case of cardiac arrest.
- Watch for urinary tract infection, and remove bladder catheter as soon as possible.
- Employ intensive pulmonary hygiene because incidence of pulmonary edema and infection is high.
- Provide meticulous wound care.
- Offer high-carbohydrate feedings because carbohydrates have a greater protein-sparing power and provide additional calories.
- Institute seizure precautions. Provide padded side rails and have airway and suction equipment at the bedside.
- Encourage and assist the patient to turn and move because drowsiness and lethargy may reduce activity.
- Explain that the patient may experience residual defects in kidney function for a long time after acute illness.
- Encourage the patient to report routine urinalysis and follow-up examinations.
- Recommend resuming activity gradually because muscle weakness will be present from excessive catabolism.
Documentation Guidelines
- Physical findings:Urinary output and description of urine, fluid balance, vital signs, findings related to original disease process or insult,presence of pain or pruritus,mental status,GI status, and skin integrity
- Condition of peritoneal or vascular access sites
- Nutrition: Response to dietary or fluid restrictions, tolerance to food, maintenance of body weight
- Complications:Cardiovascular,integumentary infection
Discharge and Home Healthcare Guidelines
All patients with ARF need an understanding of renal function,signs and symptoms of renal failure ,and how to monitor their own renal function. Patients who have recovered viable renal function still need to be monitored by a nephrologist for at least a year. Teach the patient that she or he may be more susceptible to infection than previously. Advise daily weight checks. Emphasize rest to prevent overexertion. Teach the patient or significant others about all medications, including dosage, potential side effects, and drug interactions. Explain that the patient should tell the healthcare professional about the medications if the patient needs treatment such as dental work or if a new medication is added. Explain that ongoing medical assessment is required to check renal function. Explain all dietary and fluid restrictions. Note if the restrictions are life-long or temporary.
Patients who have not recovered viable renal function need to understand that their condition may persist and even become chronic. If chronic renal failure is suspected, further outpatient treatment and monitoring are needed. Discuss with significant others the lifestyle changes that may be required with chronic renal failure.
Sources:
Nursingcrib.com
Marilyn Sawyer Sommers, RN, PhD, FAAN , Susan A. Johnson, RN, PhD, Theresa A. Beery, PhD, RN , DISEASES AND DISORDERS A Nursing Therapeutics Manual, 2007 3rd ed
Exam
Nursing Care Plan
Nursing Diagnosis: Excess fluid volume
May be relate to
- Compromised regulatory mechanism (renal failure)
Possibly evidenced by
- Intake greater than output, oliguria; changes in urine specific gravity
- Venous distension; blood pressure (BP)/central venous pressure (CVP) changes
- Generalized tissue edema, weight gain
- Changes in mental status, restlessness
- Decreased Hb/hematocrit (Hct), altered electrolytes; pulmonary congestion on x-ray
Desired Outcomes
- Display appropriate urinary output with specific gravity/laboratory studies near normal; stable weight, vital signs within patient’s normal range; and absence of edema.
Nursing Interventions
- Accurately record intake and output (I&O) noting to include “hidden” fluids such as IV antibiotic additives, liquid medications, frozen treats, ice chips. Religiously measure gastrointestinal losses and estimate insensible losses (sweating), including wound drainage, nasogastric outputs, and diarrhea.
- Rationale: Decrease in output (to less than 400 ml per 24 hours) may indicate acute failure, especially in high-risk patients. Accurate monitoring of I&O is necessary for determining renal function and fluid replacement needs and reducing risk of fluid overload. Do note that hypervolemia usually occurs in anuric phase of ARF and may mask the symptoms.
- Monitor urine specific gravity.
- Rationale: Measures the kidney’s ability to concentrate urine. In intrarenal failure, specific gravity is usually equal to or less than 1.010, indicating loss of ability to concentrate the urine.
- Weigh daily at same time of day, on same scale, with same equipment and clothing.
- Rationale: Daily body weight is best monitor of fluid status. A weight gain of more than 0.5 kg/day suggests fluid retention.
- Assess skin, face, dependent areas for edema. Evaluate degree of edema (on scale of +1–+4).
- Rationale: Edema occurs primarily in dependent tissues of the body, (hands, feet, lumbosacral area). Patient can gain up to 10 lb (4.5 kg) of fluid before pitting edema is detected. Periorbital edema may be a presenting sign of this fluid shift because these fragile tissues are easily distended by even minimal fluid accumulation.
- Monitor heart rate (HR), BP, and JVD/CVP.
- Rationale: Tachycardia and hypertension can occur because of: (1) failure of the kidneys to excrete urine, (2) excess fluid resuscitation during efforts to treat hypovolemia and/or hypotension or convert oliguric phase of renal failure, (3) changes in the renin-angiotensin system. Invasive monitoring may be needed for assessing intravascular volume, especially in patients with poor cardiac function.
- Auscultate lung and heart sounds.
- Rationale: Fluid overload may lead to pulmonary edema and HF evidenced by development of adventitious breath sounds, extra heart sounds.
- Assess level of consciousness. Investigate changes in mentation, presence of restlessness.
- Rationale: May reflect fluid shifts, accumulation of toxins, acidosis, electrolyte imbalances, or developing hypoxia.
- Scatter desired beverages throughout the 24-hour period and give various offering (hot, cold, frozen).
- Rationale: Helps avoid periods without fluids, minimizes boredom of limited choices, and reduces sense of deprivation and thirst.
- Correct any reversible cause of ARF: replace blood loss, maximize cardiac output, discontinue nephrotoxic drug, relieve obstruction via surgery.
- Rationale: Kidneys may be able to return to normal functioning, preventing or limiting residual effects.
- Use appropriate safety measures (raising side rails and restraints.
- Rationale: Patient with CNS involvement may be dizzy and/or confused.
Monitor diagnostic studies:
- Blood urea nitrogen (BUN), creatinine (cr)
- Rationale: BUN assess management of renal dysfunction. Both values may increase but creatinine is a better indicator of renal function because it is not affected by hydration, diet, and tissue catabolism. Dialysis is usually indicated if ratio is higher than 10:1 or if therapy fails to indicate fluid overload or metabolic acidosis.
- Urine sodium and Cr.
- Rationale: In ATN, tubular functional integrity is lost and sodium resorption is impaired, resulting in increased sodium excretion. Urine creatinine is usually decreased as serum creatinine elevates.
- Serum sodium.
- Rationale: Hyponatremia may result from fluid overload (dilutional) or kidney’s inability to conserve sodium. Hypernatremia indicates total body water deficit.
- Serum potassium.
- Rationale: Lack of renal excretion and/or selective retention of potassium to excrete excess hydrogen ions leads to hyperkalemia, requiring prompt intervention.
- Hb/Hct.
- Rationale: Decreased values may indicate hemodilution (hypervolemia) however, during prolonged failure, anemia frequently develops as a result of RBC loss. Other possible causes (active or occult hemorrhage) should also be evaluated.
- Serial chest x-rays.
- Rationale: Increased cardiac size, prominent pulmonary vascular markings, pleural effusion, congestion indicate acute responses to fluid overload or chronic changes associated with renal and heart failure.
- Administer and/or restrict fluids as indicated.
- Rationale: Fluid management is usually calculated to replace output from all sources plus estimated insensible losses (metabolism, diaphoresis). Prerenal failure (azotemia) is treated with volume replacement and/or vasopressors. The oliguric patient with adequate circulating volume or fluid overload who is unresponsive to fluid restriction and diuretics requires dialysis. Note: During oliguric phase, “push/pull” therapy (push IV fluids and diurese with diuretics) may be tried to stimulate kidney function.
Administer medication as indicated:
- Diuretics: furosemide (Lasix), bumetanide (Bumex), torsemide (Demadex), mannitol (Osmitrol).
- Rationale: Given early in oliguric phase of ARF in an effort to convert to non-oliguric phase, flush the tubular lumen of debris, reduce hyperkalemia, and promote adequate urine volume.
- Antihypertensives: clonidine (Catapres), methyldopa (Aldomet), prazosin (Minipress).
- Rationale: May be given to treat hypertension by counteracting effects of decreased renal blood flow and/or circulating volume overload.
- Calcium channel blockers.
- Rationale: Given early in nephrotoxic ATN to reduce influx of calcium into kidney cells, thereby helping to maintain cell integrity and improve GFR.
- Prostaglandins.
- Rationale: Vasodilatory effect may improve circulating volume and reestablish renal blood flow to aid in clearing nephrotoxic agents from nephrons.
- Insert indwelling catheter, as indicated.
- Rationale: Catheterization excludes lower tract obstruction and provides means of accurate monitoring of urine output during acute phase; however, indwelling catheterization may be contraindicated because of increased risk of infection.
- Prepare for dialysis as indicated: hemodialysis, peritoneal dialysis, or continuous renal replacement therapy (CRRT).
- Rationale: Done to correct volume overload, electrolyte and acid-base imbalances, and to remove toxins. The type of dialysis chosen for ARF depends on the degree of hemodynamic compromise and patient’s ability to withstand the procedure.
- During peritoneal dialysis, position the patient carefully: elevate the head of the bed.
- Rationale: Doing so would reduce the pressure on the diaphragm and can aid in respiration.
- Watch out for complications such as peritonitis, atelectasis, hypokalemia, pneumonia and/or shock.
- Rationale: These complications are common for patients undergoing peritoneal dialysis.
Nursing Diagnosis: Risk for decreased cardiac output
Risk factors may include
- Fluid overload (kidney dysfunction/failure, overzealous fluid replacement)
- Fluid shifts, fluid deficit (excessive losses)
- Electrolyte imbalance (potassium, calcium); severe acidosis
- Uremic effects on cardiac muscle/oxygenation
Possibly evidenced by
- Not applicable. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.
Desired Outcomes
- Maintain cardiac output as evidenced by BP and HR/rhythm within patient’s normal limits; peripheral pulses strong and equal with adequate capillary refill time.
Nursing Interventions
- Monitor BP and HR.
- Rationale: Fluid volume excess, combined with hypertension (common in renal failure) and effects of uremia, increases cardiac workload and can lead to cardiac failure. In ARF, cardiac failure is usually reversible.
- Observe ECG or telemetry for changes in rhythm.
- Rationale: Changes in electromechanical function may become evident in response to progressing renal failure and accumulation of toxins and electrolyte imbalance. Peaked T wave, wide QRS, prolonged PR interval is usually associated with hyperkalemia. Flat T wave, peaked P wave, and appearance of the U waves usually indicate hypokalemia. Prolonged QT interval may reflect calcium deficit.
- Auscultate heart sounds.
- Rationale: Development of S3/S4 is indicative of failure. Pericardial friction rub may be only manifestation of uremic pericarditis, requiring prompt intervention and possibly acute dialysis.
- Assess color of skin, mucous membranes, and nail beds. Note capillary refill time.
- Rationale: Pallor may reflect vasoconstriction or anemia. Cyanosis is a late sign and is related to pulmonary congestion and/or cardiac failure.
- Note occurrence of slow pulse, hypotension, flushing, nausea and vomiting, and depressed level of consciousness.
- Rationale: Use of drugs (like antacids) containing magnesium can result in hypermagnesemia, potentiating the neuromuscular dysfunction and risk of a respiratory or cardiac arrest. Use aluminum-hydroxide-based antacid.
- Monitor for GI bleeding by guaiac testing all stools for blood.
- Rationale: Gastrointestinal bleeding is a known complication of renal failure; however, its pathogenesis remains uncertain. Some have attributed gastrointestinal bleeding to the effects of uremia on the gastrointestinal mucosa; others have suggested that uremia may affect platelet adhesiveness, which may explain the prolonged gastrointestinal bleeding seen in patients with renal failure. In addition, the role of heparinization and the widespread use of antiplatelet agents in patients on dialysis have been implicated in the etiology of gastrointestinal bleeding.
- Investigate reports of muscle cramps, numbness of fingers, with muscle twitching, hyperreflexia.
- Rationale: Neuromuscular indicators of hypocalcemia, which can also affect cardiac contractility and function.
- Maintain bed rest or encourage adequate rest and provide assistance with care and desired activities.
- Rationale: Reduces oxygen consumption and cardiac workload.
Monitor laboratory studies:
- Potassium.
- Rationale:During oliguric phase, hyperkalemia is present but often shifts to hypokalemia in diuretic or recovery phase. Any potassium value associated with ECG changes requires intervention. Note: A serum level of 6.5 mEq or higher constitutes a medical emergency.
- Calcium.
- Rationale: In addition to its own cardiac effects, calcium deficit enhances the toxic effects of potassium.
- Magnesium.
- Rationale: Dialysis or calcium administration may be necessary to combat the CNS-depressive effects of an elevated serum magnesium level.
- Administer and/or restrict fluids as indicated.
- Rationale: Cardiac output depends on circulating volume (affected by both fluid excess and deficit) and myocardial muscle function.
- Provide supplemental oxygen if indicated.
- Rationale: Maximizes available oxygen for myocardial uptake to reduce cardiac workload and cellular hypoxia.
Administer medications as indicated:
- Inotropic agents: digoxin (Lanoxin)
- Rationale: May be used to improve cardiac output by increasing myocardial contractility and stroke volume. Dosage depends on renal function and potassium balance to obtain therapeutic effect without toxicity.
- Calcium gluconate
- Rationale: Serum calcium is often low but usually does not require specific treatment in ARF. Calcium gluconate may be given to treat hypocalcemia and to offset the effects of hyperkalemia by modifying cardiac irritability.
- Aluminum hydroxide gels (Amphojel, Basaljel)
- Rationale: Increased phosphate levels may occur as a result of failure of glomerular filtration and require use of phosphate-binding antacids to limit phosphate absorption from the GI tract.
- Glucose and/or insulin solution
- Rationale: Temporary measure to lower serum potassium by driving potassium into cells when cardiac rhythm is endangered.
- Sodium bicarbonate or sodium citrate
- Rationale: May be used to correct acidosis or hyperkalemia (by increasing serum pH) if patient is severely acidotic and not suffering from fluid overload.
- Sodium polystyrene sulfonate (Kayexalate) with or without sorbitol.
- Rationale: Exchange resin trades sodium for potassium in the GI tract to lower serum potassium level. Sorbitol may be included to cause osmotic diarrhea to help excrete potassium.
- Prepare for/assist with dialysis as necessary.
- Rationale: May be indicated for persistent dysrhythmias, progressive HF unresponsive to other therapies.
Nursing Diagnosis: Nutrition: imbalanced, risk for less than body requirements
Risk factors may include
- Protein catabolism; dietary restrictions to reduce nitrogenous waste products
- Increased metabolic needs
- Anorexia, nausea/vomiting; ulcerations of oral mucosa
Possibly evidenced by
- Not applicable. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.
Desired Outcomes
- Maintain/regain weight as indicated by individual situation, free of edema.
Nursing Interventions
- Assess and document dietary intake.
- Rationale: Aids in identifying deficiencies and dietary needs. General physical condition, uremic symptoms (nausea, anorexia), and multiple dietary restrictions affect food intake.
- Provide frequent, small feedings.
- Rationale: Minimizes anorexia and nausea associated with uremic state and/or diminished peristalsis.
- Give patient/SO a list of permitted foods or fluids and encourage involvement in menu choices.
- Rationale: Provides patient with a measure of control within dietary restrictions. Food from home may enhance appetite.
- Offer frequent mouth care or rinse with diluted acetic acid solution. Give gums, hard candy, breath mints between meals.
- Rationale: Mucous membranes may become dry and cracked. Mouth care soothes, lubricates, and helps freshen mouth taste, which is often unpleasant because of uremia and restricted oral intake. Rinsing with acetic acid helps neutralize ammonia formed by conversion of urea.
- Weigh daily.
- Rationale: The fasting or catabolic patient normally loses 0.2–0.5 kg/day. Changes in excess of 0.5 kg may reflect shifts in fluid balance.
- Monitor laboratory studies: BUN, albumin, transferrin, sodium, and potassium.
- Rationale: Indicators of nutritional needs, restrictions, and necessity for and effectiveness of therapy.
- Consult with dietitian support team.
- Rationale: Determines individual calorie and nutrient needs within the restrictions, and identifies most effective route and product (oral supplements, enteral or parenteral nutrition).
- Provide high-calorie, low to moderate protein diet. Include complex carbohydrates and fat sources to meet caloric needs and essential amino acids. Avoid concentrated sugar sources. Give anorectic patients small, frequent meals.
- Rationale: The amount of needed exogenous protein is less than normal unless patient is on dialysis. Carbohydrates meet energy needs and limit tissue catabolism, preventing keto acid formation from protein and fat oxidation. Carbohydrate intolerance mimicking DM may occur in severe renal failure. Essential amino acids improve nitrogen balance and nutritional status, stimulate repair of tubular epithelial cells, and enhance patient’s ability to fight systemic complications.
- Maintain proper electrolyte balance by strictly monitoring levels.
- Rationale: Medications and decrease in GFR can cause electrolyte imbalances and may further cause renal injury.
- Restrict potassium, sodium, and phosphorus intake as indicated.
- Rationale: Restriction of these electrolytes may be needed to prevent further renal damage, especially if dialysis is not part of treatment, and/or during recovery phase of ARF.
Administer medications as indicated:
- Iron preparations
- Rationale: Iron deficiency may occur if protein is restricted, patient is anemic, or GI function is impaired.
- Calcium carbonate
- Rationale: Restores normal serum levels to improve cardiac and neuromuscular function, blood clotting, and bone metabolism. Note: Low serum calcium is often corrected as phosphate absorption is decreased in the GI system. Calcium may be substituted as a phosphate binder.
- Vitamin D
- Rationale: Necessary to facilitate absorption of calcium from the GI tract.
- B complex and C vitamins, folic acid
- Rationale: Vital as coenzyme in cell growth and actions. Intake is decreased because of protein restrictions.
- Antiemetics: prochlorperazine (Compazine), trimethobenzamide (Tigan).
- Rationale: Given to relieve N/V and may enhance oral intake.
Nursing Diagnosis: Risk for Infection
Risk factors may include
- Depression of immunologic defenses (secondary to uremia)
- Invasive procedures/devices (e.g., urinary catheterization)
- Changes in dietary intake/malnutrition
Possibly evidenced by
- Not applicable. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.
Desired Outcomes
- Experience no signs/symptoms of infection.
Nursing Interventions
- Promote good hand washing by patient and staff.
- Rationale: Reduces risk of cross contamination.
- Avoid invasive procedures, instrumentation, and manipulation of indwelling catheters whenever possible. Use aseptic technique when caring and manipulating IV and invasive lines. Change site dressings per protocol. Note edema, purulent drainage.
- Rationale: Limits introduction of bacteria into body. Early detection of developing infection may prevent sepsis.
- Provide routine catheter care and promote meticulous perineal care. Keep urinary drainage system closed and remove indwelling catheter as soon as possible.
- Rationale: Reduces bacterial colonization and risk of ascending UTI.
- Encourage deep breathing, coughing, frequent position changes.
- Rationale: Prevents atelectasis and mobilizes secretions to reduce risk of pulmonary infections.
- Assess skin integrity.
- Rationale: Excoriations from scratching may become secondarily infected.
- Monitor vital signs.
- Rationale: Fever (higher than 100.4°F) with increased pulse and respirations is typical of increased metabolic rate resulting from inflammatory process, although sepsis can occur without a febrile response.
- Monitor laboratory studies: WBC count with differential.
- Rationale: Although elevated WBCs may indicate generalized infection, leukocytosis is commonly seen in ARF and may reflect injury within the kidney. A shifting of the differential to the left is indicative of infection.
- Obtain specimen(s) for culture and sensitivity and administer appropriate antibiotics as indicated.
- Rationale: Verification of infection and identification of specific organism aids in choice of the most effective treatment. Note: A number of anti-infective agents require adjustments of dose and/or time while renal clearance is impaired.
Nursing Diagnosis: Risk for Deficient Fluid Volume
Risk factors may include
- Excessive loss of fluid (diuretic phase of ARF, with rising urinary volume and delayed return of tubular reabsorption capabilities)
Possibly evidenced by
- Not applicable. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.
Desired Outcomes
- Display I&O near balance; good skin turgor, moist mucous membranes, palpable peripheral pulses, stable weight and vital signs, electrolytes within normal range.
Nursing Interventions
- Measure I&O accurately. Weigh daily. Calculate insensible fluid losses.
- Rationale: Assessment can help estimate fluid replacement needs. Fluid intake should approximate losses through urine, nasogastric or wound drainage, and insensible water losses (diaphoresis, metabolism).
- Provide allowed fluids throughout 24-hr period.
- Rationale: Diuretic phase of ARF may revert to oliguric phase if fluid intake is not maintained or nocturnal dehydration occurs.
- Monitor BP (noting postural changes) and HR.
- Rationale: Orthostatic hypotension and tachycardia suggest hypovolemia.
- Note signs and symptoms of dehydration: dry mucous membranes, thirst, dulled sensorium, peripheral vasoconstriction.
- Rationale: In diuretic or postobstructive phase of renal failure, urine output can exceed 3 L/day. Extracellular fluid volume depletion activates the thirst center, and sodium depletion causes persistent thirst, unrelieved by drinking water. Continued fluid losses including inadequate replacement may lead to hypovolemic state.
- Control environmental temperature; limit bed linens as indicated.
- Rationale:May reduce diaphoresis, which contributes to overall fluid losses.
- Monitor laboratory studies
- Rationale: In nonoliguric ARF or in diuretic phase of ARF, large urine losses may result in sodium wasting while elevated urinary sodium acts osmotically to increase fluid losses. Restriction of sodium may be indicated to break the cycle.
Nursing Diagnosis: Deficient Knowledge
May be related to
- Lack of exposure/recall
- Information misinterpretation
- Unfamiliarity with information resources
Possibly evidenced by
- Questions/request for information, statement of misconception
- Inaccurate follow-through of instructions/development of preventable
- Complications
Desired Outcomes
- Verbalize understanding of condition/disease process, prognosis, and potential complications.
- Identify relationship of signs/symptoms to the disease process and correlate symptoms with causative factors.
- Verbalize understanding of therapeutic needs.
- Initiate necessary lifestyle changes and participate in treatment regimen.
Nursing Interventions
- Review disease process, prognosis, and precipitating factors if known.
- Rationale: Provides knowledge base from which patient can make informed choices.
- Explain level of renal function after acute episode is over.
- Rationale: Patient may experience residual defects in kidney function, which may or may not be permanent.
- Discuss renal dialysis or transplantation if these are likely options for the future.
- Rationale: Although these options would have been previously presented by the physician, patient may now be at a point when options need to be considered and may desire additional input.
- Review dietary plan and restrictions. Include fact sheet listing food restrictions.
- Rationale: Adequate nutrition is necessary to promote tissue healing; adherence to restrictions may prevent complications.
- Encourage patient to observe characteristics of urine and amount, frequency of output.
- Rationale:Changes may reflect alterations in renal function and need for dialysis.
- Establish regular schedule for weighing.
- Rationale: Useful tool for monitoring fluid and dietary needs.
- Provide emotional support to the patient and family.
- Rationale: To reassure them of the all the procedures that patient may undergo.
- Review fluid restriction. Remind patient to spread fluids over entire day and to include all fluids (ice) in daily fluid counts.
- Rationale: Depending on the cause and stage of ARF, patient may need to either restrict or increase intake of fluids.
- Discuss activity restriction and gradual resumption of desired activity. Encourage use of energy-saving, relaxation, and diversional techniques.
- Rationale: Patient with severe ARF may need to restrict activity and/or may feel weak for an extended period during lengthy recovery phase, requiring measures to conserve energy and reduce boredom.
- Discuss reality of continued presence of fatigue.
- Rationale: Decreased metabolic energy production, presence of anemia, and states of discomfort commonly result in fatigue.
- Determine ADLs and personal responsibilities. Identify available resources and support systems.
- Rationale: Helps patient manage lifestyle changes and meet personal needs.
- Recommend scheduling activities with adequate rest periods.
- Rationale: Prevents excessive fatigue and conserves energy for healing, tissue regeneration.
- Review use of medication. Encourage patient to discuss all medications and herbal supplements with physician.
- Rationale: Medications that are concentrated in and/or excreted by the kidneys can cause toxic cumulative reactions and/or permanent damage to kidneys. Some supplements may interact with prescribed medications and may electrolytes.
- Stress necessity of follow-up care, laboratory studies.
- Rationale: Renal function may be slow to return following acute failure (up to 12 mo), and deficits may persist, requiring changes in therapy to avoid recurrence.
- Identify symptoms requiring medical intervention: decreased urinary output, sudden weight gain, presence of edema, lethargy, bleeding, signs of infection, altered mentation.
- Rationale: Prompt evaluation and intervention may prevent serious complications or progression to chronic renal failure.
Other Possible Nursing Care Plans
- Fluid Volume, deficient (specify)—dependent on cause, duration, and stage of recovery.
- Fatigue—decreased metabolic energy production/dietary restriction, anemia, increased energy requirements, e.g., fever/inflammation, tissue regeneration.
- Infection, risk for—depression of immunologic defenses (secondary to uremia), changes in dietary intake/malnutrition, increased environmental exposure.
- Therapeutic Regimen: ineffective management—complexity of therapeutic regimen, economic difficulties, perceived benefit.

