Notes
Description
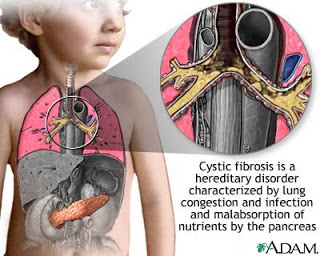
- Is an autosomal recessive disorder affecting the exocrine glands, in which their secretions become abnormally viscous and liable to obstruct glandular ducts.
- It primarily affects pulmonary and GI function.
- The average life expectancy for the cystic fibrosis patient is currently age 30 to 40. Death may occur because of respiratory infection and failure.
- Other complications include esophageal varices, diabetes, chronic sinusitis, pancreatitis, rectal polyps, intussusceptions, growth retardation, and infertility.
Causes/ Risk Factors
- The responsible gene,the CF transmembrane conductance regulator (CFTR),is mapped to chromosome 7 (see Genetic Considerations). The underlying defect of this autosomal recessive condition involves a defective protein that interferes with chloride transport, which, in turn, makes the body’s secretions very thick and tenacious. The ducts of the exocrine glands subsequently become obstructed.
Assessment
- Usually present before age 6 months but severity varies and may present later.
- Meconium ileus is found in neonate.
- Usually present with respiratory symptoms, chronic cough, and wheezing.
- Parents may report salty taste when skin is kissed.
- Recurrent pulmonary infections.
- Failure to gain weight or grow in the presence of a good appetite.
- Frequent, bulky, and foul smelling stools (steatorrhea), excessive flatus, pancreatitis and obstructive jaundice may occur.
- Protuberant abdomen, pot belly, wasted buttocks.
- Bleeding disorders.
- Clubbing of fingers in older child.
- Increased anteroposterior chest diameter (barrel chest).
- Decreased exertional endurance.
- Hyperglycemia, glucosuria with polyuria, and weight loss.
- Sterility in males.
Diagnostic Evaluation
- Sweat chloride test measures sodium and chloride level in sweat.
- Chloride level of more than 60 mEq/L is virtually diagnostic.
- Chloride level of 40 to 60 mEq/L is borderline and should be repeated.
- Duodenal secretions: low trypsin concentration is virtually diagnostic.
- Stool analysis:
- Reduced trypsin and chymotrypsin levels-used for initial screening for cystic fibrosis.
- Increased stool fat concentration.
- BMC ( Boehringer-Mannheim Corp.) meconium strip test for stool includes lactose and protein content; used for screening.
- Chest X-ray may be normal initially; later shows increased areas of infection, overinflation, bronchial thickening and plugging, atelectasis, and fibrosis.
- Pulmonary function studies (after age 4) show decreased vital capacity and flow rates and increased residual volume or increased total lung capacity.
- Diagnosis is made when a positive sweat test is seen in conjunction with one or more of the following:
- Positive family history of cystic fibrosis.
- Typical chronic obstructive lung disease.
- Documented exocrine pancreatic insufficiency.
- Genetic screening may be done for affected families.
Primary Nursing Diagnosis
- Ineffective airway clearance related to excess tenacious mucus
Therapeutic Intervention / Medical Management
Treatment for lung problems includes:
- Antibiotics to prevent and treat lung and sinus infections. They may be taken by mouth, or given in the veins or by breathing treatments. People with cystic fibrosis may take antibiotics only when needed, or all the time. Doses are usually higher than normal.
- Inhaled medicines to help open the airways
- DNAse enzyme replacement therapy to thin mucus and make it easier to cough up
- Flu vaccine and pneumococcal polysaccharide vaccine (PPV) yearly (ask your health care provider)
- Lung transplant is an option in some cases
- Oxygen therapy may be needed as lung disease gets worse
Treatment for bowel and nutritional problems may include:
- A special diet high in protein and calories for older children and adults (see: Cystic fibrosis nutrional considerations)
- Pancreatic enzymes to help absorb fats and protein
- Vitamin supplements, especially vitamins A, D, E, and K
- Your doctor can suggest other treatments if you have very hard stools
Pharmacologic Intervention
- Antimicrobial therapy as indicated for pulmonary infection.
- Oral or I.V. antibiotics as required.
- Inhaled antibiotics, such as gentamicin or tobramycin, may be used for severe lung disease or colonization of organisms.
- Bronchodilators to increase airway size and assist in mucus clearance.
- Pulmozyme recombinant human DNase (an enzyme) administered via nebulization to decrease viscosity of secretions.
- Pancreatic enzyme supplements with each feeding.
- Favored preparation is pancrelipase.
- Occasionally, antacid is helpful to improve tolerance of enzymes.
- Favorable response to enzymes is based on tolerance of fatty foods, decreased stool frequency, absence of steatorrhea, improved appetite, and lack of abdominal pain.
- Gene therapy, in which recombinant DNA containing a corrected gene sequence is introduced into the diseased lung tissue by nebulization, is in clinical trials.
Nursing Intervention
- Monitor weight at least weekly to assess effectiveness of nutritional interventions.
- Monitor respiratory status and sputum production, to evaluate response to respiratory care measures.
- To promote airway clearance, employ intermittent aerosol therapy three to four times per day when the child is symptomatic.
- Perform chest physical therapy three to four times per day after aerosol therapy.
- Help the child to relax to cough more easily after postural drainage.
- Suction the infant or young child when necessary, if not able to cough.
- Teach the child breathing exercises using pursed lips to increase duration of exhalation.
- Provide good skin care and position changes to prevent skin breakdown in malnourished child.
- Provide frequent mouth care to reduce chances of infection because mucus is present.
- Restrict contact with people with respiratory infection.
- Encourage diet composed of foods high in calories and protein and moderate to high in fat because absorption of food is incomplete.
- Administer fat-soluble vitamins, as prescribed, to counteract malabsorption.
- Increase salt intake during hot weather, fever, or excessive exercise to prevent sodium depletion and cardiovascular compromise.
- To prevent vomiting, allow ample time for feeding because of irritability if not feeling well and coughing.
- Encourage regular exercise and activity to foster sense of accomplishments and independence and improve pulmonary function.
- Provide opportunities for parents to learn all aspects of care for the child.
- Teach the parents about dietary regimen and special need for calories, fat, and vitamins.
- Discuss need for salt replacement, especially on hot summer days or when fever, vomiting, and diarrhea occur.
Documentation Guidelines
- Physical response: Pulmonary assessment; color, odor, character of mucus; cardiac and GI assessment; pulse oximetry
- Nutritional data:Weight,use of enzymes,adherence to supplemental feedings
- Emotional response: Patient’s feelings about dealing with a chronic illness, patient’s body image,parents’coping ability,siblings’response
Discharge and Home Healthcare Guidelines
Teach the patient and family how to prevent future episodes of pneumonia through CPT,expectoration of sputum, and avoidance of peers with common colds and nasopharyngitis. Explain that medications need to be taken at the time of each meal, especially pancreatic enzymes and supplemental vitamins. Teach the parents protocols for home IV care, as needed. Teach parents when to contact the physician:when temperature is elevated over 100.5°F, sputum has color to it, or the child complains of increased lung congestion or abdominal pain. Also educate parents on the need to keep routine follow-up appointments for medication,laboratory, and general checkups. Teach the patient or parents proper insulin administration and the appropriate signs and symptoms of high and low glucose levels.
Sources:
http://www.nlm.nih.gov/medlineplus/ency/article/000107.htm
Nursingcrib.com
Marilyn Sawyer Sommers, RN, PhD, FAAN , Susan A. Johnson, RN, PhD, Theresa A. Beery, PhD, RN , DISEASES AND DISORDERS A Nursing
Therapeutics Manual, 2007 3rd ed
Exam
Nursing Care Plan
Nursing Diagnosis
Ineffective airway clearance related to thick mucus secretions and effort and a lot of bad cough.
Goal: Not experiencing aspiration.
Outcomes
- Shows an effective cough and increased air exchange in the lungs.
Interventions
- Auscultation of breath sounds. Note the example of wheezing breath sounds, crackles, rhonchi.
- Rationale: Some degree of spasm of the bronchial obstruction with airway obstruction and may / not indicated the presence of abnormal breath sounds or crackles eg absence of breath sounds.
- Perform physiotherapy to issue secret and give the patient a comfortable position, eg, elevation of the head of the bed, sitting on the back of the bed (position semi-Fowler / Fowler).
- Rationale: head of bed elevation facilitate respiratory function using gravity.
- Assist clients to dilute sputum, with the collaboration expectorant administration to improve airway clearance.
- Rationale: Giving expectorants may help thin the secret, that secret is more easily removed.
- Provide nebulizer with a solution and in accordance with the right tools.
- Rationale: Nebulization can help spending viscous secretions.
- Observations clients closely after aerosol therapy and chest physiotherapy to preventaspiration due to many sputum suddenly become watery.
- Rationale: To prevent aspiration.
- Provide postural drainage (adjust the area where there is a buildup of mucus) as prescribed to reduce the viscosity of mucus.
- Rationale: Postural drainage aids in the excretion of mucus is thick.
Nursing Diagnosis
- Impaired gas exchange related to airway obstruction by nasal obstruction.
Goal: Maintaining adequate oxygenation or ventilation.
Outcomes
- The patient showed respiratory rate effectively.
- Free of respiratory distress.
- Arterial blood gas within the normal range.
Nursing Interventions
- Maintain a patent airway.
- Rationale: Preventing complications of respiratory failure.
- Position the patient to obtain maximum efficiency ventilators, such as a high Fowler’s position or sitting, leaning forward.
- Rationale: Position Fowler / semi-Fowler can facilitate respiratory function and can reduce airway collapse, dyspnoea, and breath work by using gravity.
- Monitor vital signs, arterial blood gases (ABGs), and pulse oximetry to detect / prevent hypoxemia.
- Rationale: increased PaCO2 indicates impending respiratory failure during asthmatic. Tachycardia, dysrhythmias, and changes in BP may indicate systemic hypoxemia effects on cardiac function.
- Provide supplemental oxygen according to the provisions / requirements. Monitor patients closely for carbon dioxide narcosis due to oxygen is danger of oxygen therapy in patients with chronic lung disease.
- Rationale: Occurrence / respiratory failure that would require effort dating lifesaving action. Supplemental oxygen administration can fix / prevent worsening hypoxia.
- Motivation exercise appropriate physical condition of the patient.
- Rationale: Physical exercise is often effective to clear accumulated lung secretions and to improve endurance exercise capacity before experiencing dyspnea
Nursing Diagnosis
- Ineffective breathing pattern related to tracheobronchial obstruction.
Goal:
- Repairing or maintaining a normal breathing pattern.
- Patients achieving lung function maximum.
Outcomes
- Patients showed an effective respiratory frequency with the frequency and depth within the normal range and lungs clear / clean.
- Patients free of dyspnea, cyanosis, or other signs of respiratory distress.
Nursing Interventions
- Provide position Fowler or semi-Fowler.
- Rationale: Position Fowler / semi-Fowler enables lung expansion and ease breathing. Changing position and ambulation improve air charging different lung segments which improves gas diffusion.
- Teach deep breathing techniques, and or lip breathing or diaphragmatic breathingabdominal exercises when indicated and effective cough.
- Rationale: to help spending sputum.
- Observation vital signs (RR or frequency per minute).
- Rationale: Tachycardia, dysrhythmias, and changes in BP may indicate the effect of systemic hypoxemia pad cardiac function.

