Notes
Description
- Diabetes is a chronic disease, which occurs when the pancreas does not produce enough insulin, or when the body cannot effectively use the insulin it produces. This leads to an increased concentration of glucose in the blood (hyperglycaemia).
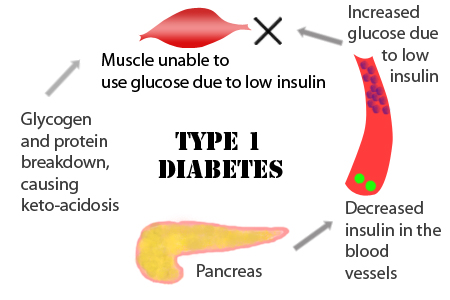
- Type 1 diabetes (previously known as insulin-dependent or childhood-onset diabetes) is characterized by a lack of insulin production.
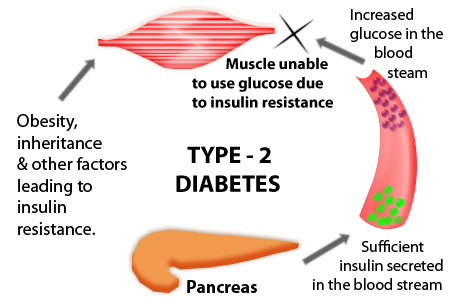
- Type 2 diabetes (formerly called non-insulin-dependent or adult-onset diabetes) is caused by the body’s ineffective use of insulin. It often results from excess body weight and physical inactivity.
- Gestational diabetes is hyperglycaemia that is first recognized during pregnancy.
Causes
The cause of diabetes depends on the type.
Type 1 diabetes
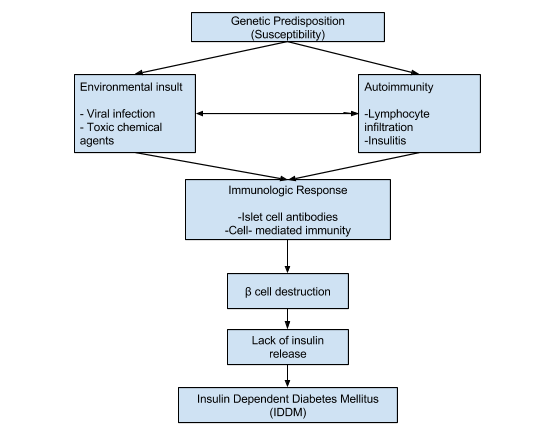
- Is partly inherited, and then triggered by certain infections, with some evidence pointing at Coxsackie B4 virus. A genetic element in individual susceptibility to some of these triggers has been traced to particular HLA genotypes (i.e., the genetic “self” identifiers relied upon by the immune system). However, even in those who have inherited the susceptibility, type 1 DM seems to require an environmental trigger. The onset of type 1 diabetes is unrelated to lifestyle.

Type 2 diabetes
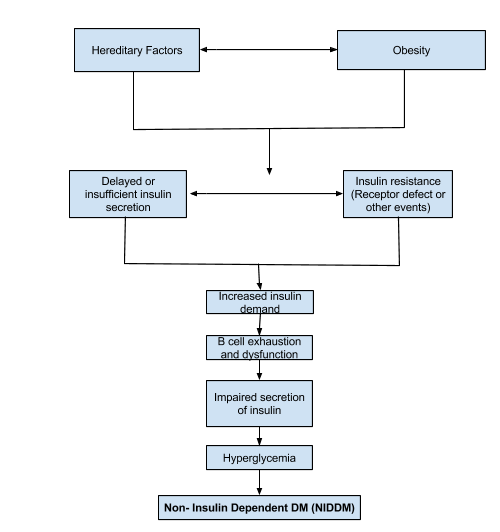
- is due primarily to lifestyle factors and genetics.
The following is a comprehensive list of other causes of diabetes:
- Genetic defects of β-cell function
- Maturity onset diabetes of the young
- Mitochondrial DNA mutations
- Genetic defects in insulin processing or insulin action
- Defects in proinsulin conversion
- Insulin gene mutations
- Insulin receptor mutations
- Exocrine pancreatic defects
- Chronic pancreatitis
- Pancreatectomy
- Pancreatic neoplasia
- Cystic fibrosis
- Hemochromatosis
- Fibrocalculous pancreatopathy
- Endocrinopathies
- Growth hormone excess (acromegaly)
- Cushing syndrome
- Hyperthyroidism
- Pheochromocytoma
- Glucagonoma
- Infections
- Cytomegalovirus infection
- Coxsackievirus B
- Drugs
- Glucocorticoids
- Thyroid hormone
- β-adrenergic agonists
- Statins
TYPE I VERSUS TYPE 2 DIABETES
| PE I (IDDM) | TYPE 2 (NIDDM) | |
| Age of onset | Usually younger than 40 | Usually older than 40 |
| Body weight | Thin | Usually overweight |
| Symptoms | Sudden onset | Insidious onset |
| Insulin produced | None | Too little, or not effective |
| Insulin requirements | Exogenous insulin required | May require insulin |
Pathophysiology
DM Type I
DM Type II
Signs and symptoms
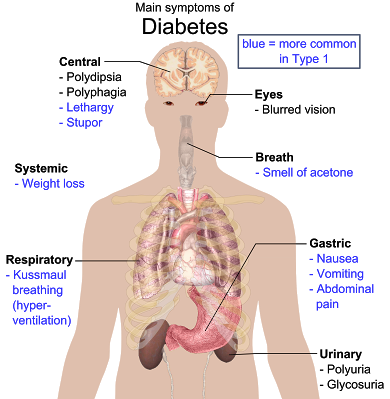
- The classic symptoms of untreated diabetes are loss of weight, polyuria (frequent urination),polydipsia (increased thirst) and polyphagia (increased hunger).Symptoms may develop rapidly (weeks or months) in type 1 diabetes, while they usually develop much more slowly and may be subtle or absent in type 2 diabetes.
- Prolonged high blood glucose can cause glucose absorption in the lens of the eye, which leads to changes in its shape, resulting in vision changes. Blurred vision is a common complaint leading to a diabetes diagnosis; type 1 should always be suspected in cases of rapid vision change, whereas with type 2 change is generally more gradual, but should still be suspected. A number of skin rashes that can occur in diabetes are collectively known as diabetic dermadromes.
Diabetic emergencies
- People (usually with type 1 diabetes) may also present with diabetic ketoacidosis, a state of metabolic dysregulation characterized by the smell of acetone, a rapid, deep breathing known as Kussmaul breathing, nausea, vomiting and abdominal pain, and altered states of consciousness.
- A rare but equally severe possibility is hyperosmolar nonketotic state, which is more common in type 2 diabetes and is mainly the result of dehydration.
WARNING SIGNS OF DIABETES
| SIGNS AND SYMPTOMSS | LABORATORY FINDINGS |
|
|
Cause: Usually secondary to excess insulin, exercise, or not enough food
Signs and Symptoms
- Nervousness
- Irritability
- Diaphoresis (heavy sweating)
- Hunger
- Weakness
- Tachycardia
- Fatigue
- Hypotension
- Palpitations
- Tachypnea
- Tremors or shaking Pallor
- Blurred or double vision
- Incoherent speech
- Headache Numbness of tongue and lips
- Confusion Coma
- Seizures
Treatment
Provide rapidly absorbed source of glucose:
- Fruit juice or cola
- Graham crackers
- Sugar cubes, sugar packets
- Hard candy
As symptoms improve:
- Provide a meal or source of complex protein or carbohydrates
HYPERGLYCEMIA
Cause: Usually secondary to insufficient insulin, illness, or excess food
Signs and Symptoms
- Confusion
- Nausea
- Irritability
- Vomiting
- Fatigue
- Anorexia
- Weakness
- Abdominal cramping
- Numbness
- Thirst
- Tachycardia
- Lethargy
- Hypotension
- Küssmall breathing
- Decreased level of consciousness
- Increased temperature
- Coma
- Flushed or dry skin
- Fruity breath
- Poor skin turgor
- Dry mucous membranes
Treatment (Requires Hospitalization)
- Restore fluid balance
- Replace electrolytes
- Lower blood glucose with regular insulin
- Monitor: Level of consciousness, vital signs, intake and output, and electrolytes
- Provide emotional support
Diagnostic Procedure
Several blood tests are used to measure blood glucose levels, the primary test for diagnosing diabetes. Additional tests can determine the type of diabetes and its severity.
- Random blood glucose test — for a random blood glucose test, blood can be drawn at any time throughout the day, regardless of when the person last ate. A random blood glucose level of 200 mg/dL (11.1 mmol/L) or higher in persons who have symptoms of high blood glucose suggests a diagnosis of diabetes.
- Fasting blood glucose test — fasting blood glucose testing involves measuring blood glucose after not eating or drinking for 8 to 12 hours (usually overnight). A normal fasting blood glucose level is less than 100 mg/dL. A fasting blood glucose of 126 mg/dL (7.0 mmol/L) or higher indicates diabetes. The test is done by taking a small sample of blood from a vein or fingertip. It must be repeated on another day to confirm that it remains abnormally high .
- Hemoglobin A1C test (A1C) — The A1C blood test measures the average blood glucose level during the past two to three months. It is used to monitor blood glucose control in people with known diabetes, but is not normally used to diagnose diabetes. Normal values for A1C are 4 to 6 percent . The test is done by taking a small sample of blood from a vein or fingertip.
- Oral glucose tolerance test — Oral glucose tolerance testing (OGTT) is the most sensitive test for diagnosing diabetes and pre-diabetes. However, the OGTT is not routinely recommended because it is inconvenient compared to a fasting blood glucose test.
The standard OGTT includes a fasting blood glucose test. The person then drinks a 75 gram liquid glucose solution (which tastes very sweet, and is usually cola or orange-flavored). Two hours later, a second blood glucose level is measured.
Oral glucose tolerance testing is routinely performed at 24 to 28 weeks of pregnancy to screen for gestational diabetes; this requires drinking a 50 gram glucose solution with a blood glucose level drawn one hour later. For women who have an abnormally elevated blood glucose level, a second OGTT is performed on another day after drinking a 100 gram glucose solution. The blood glucose level is measured before, and at one, two, and three hours after drinking the solution.
Medical Management
There is no known cure for DM. Management of the disease focuses on control of the serum glucose level to prevent or delay the development of complications. Individuals with type 1 DM require subcutaneous insulin administration. Insulin may be rapid, intermediate, or slow acting.
Patients with mild DM or those with type 2 DM or GDM may be able to control the disease by diet management alone. A diabetic diet attempts to distribute nutrition and calories throughout the 24-hour period. Daily calories consist of approximately 50% carbohydrates and 30% fat, with the remaining calories consisting of protein. The total calories allowed for an individual within the 24-hour period are based on age, weight, activity level, and medications.
In addition to strict dietary adherence to control blood glucose, obese patients with type 2 DM also need weight reduction. The dietitian selects an appropriate calorie allotment depending on the patient’s age, body size, and activity level. A useful adjunct to the management of DM is exercise. Physical activity increases the cellular sensitivity to insulin, improves tolerance to glucose, and encourages weight loss. Exercise also increases the patient’s sense of well-being concerning his or her health.
Pharmacological Highlights
When diet, exercise and maintaining a healthy weight aren’t enough, you may need the help of medication. Medications used to treat diabetes include insulin. Everyone with type 1 diabetes and some people with type 2 diabetes must take insulin every day to replace what their pancreas is unable to produce. Unfortunately, insulin can’t be taken in pill form because enzymes in your stomach break it down so that it becomes ineffective. For that reason, many people inject themselves with insulin using a syringe or an insulin pen injector,a device that looks like a pen, except the cartridge is filled with insulin. Others may use an insulin pump, which provides a continuous supply of insulin, eliminating the need for daily shots.
The most widely used form of insulin is synthetic human insulin, which is chemically identical to human insulin but manufactured in a laboratory. Unfortunately, synthetic human insulin isn’t perfect. One of its chief failings is that it doesn’t mimic the way natural insulin is secreted. But newer types of insulin, known as insulin analogs, more closely resemble the way natural insulin acts in your body. Among these are lispro (Humalog), insulin aspart (NovoLog) and glargine (Lantus).
A number of drug options exist for treating type 2 diabetes, including:
- Sulfonylurea drugs. These medications stimulate your pancreas to produce and release more insulin. For them to be effective, your pancreas must produce some insulin on its own. Second-generation sulfonylureas such as glipizide (Glucotrol, Glucotrol XL), glyburide (DiaBeta, Glynase PresTab, Micronase) and glimepiride (Amaryl) are prescribed most often. The most common side effect of sulfonylureas is low blood sugar, especially during the first four months of therapy. You’re at much greater risk of low blood sugar if you have impaired liver or kidney function.
- Meglitinides. These medications, such as repaglinide (Prandin), have effects similar to sulfonylureas, but you’re not as likely to develop low blood sugar. Meglitinides work quickly, and the results fade rapidly.
- Biguanides. Metformin (Glucophage, Glucophage XR) is the only drug in this class available in the United States. It works by inhibiting the production and release of glucose from your liver, which means you need less insulin to transport blood sugar into your cells. One advantage of metformin is that is tends to cause less weight gain than do other diabetes medications. Possible side effects include a metallic taste in your mouth, loss of appetite, nausea or vomiting, abdominal bloating, or pain, gas and diarrhea. These effects usually decrease over time and are less likely to occur if you take the medication with food. A rare but serious side effect is lactic acidosis, which results when lactic acid builds up in your body. Symptoms include tiredness, weakness, muscle aches, dizziness and drowsiness. Lactic acidosis is especially likely to occur if you mix this medication with alcohol or have impaired kidney function.
- Alpha-glucosidase inhibitors. These drugs block the action of enzymes in your digestive tract that break down carbohydrates. That means sugar is absorbed into your bloodstream more slowly, which helps prevent the rapid rise in blood sugar that usually occurs right after a meal. Drugs in this class include acarbose (Precose) and miglitol (Glyset). Although safe and effective, alpha-glucosidase inhibitors can cause abdominal bloating, gas and diarrhea. If taken in high doses, they may also cause reversible liver damage.
- Thiazolidinediones. These drugs make your body tissues more sensitive to insulin and keep your liver from overproducing glucose. Side effects of thiazolidinediones, such as rosiglitazone (Avandia) and pioglitazone hydrochloride (Actos), include swelling, weight gain and fatigue. A far more serious potential side effect is liver damage. The thiazolidinedione troglitzeone (Rezulin) was taken off the market in March 2000 because it caused liver failure. If your doctor prescribes these drugs, it’s important to have your liver checked every two months during the first year of therapy. Contact your doctor immediately if you experience any of the signs and symptoms of liver damage, such as nausea and vomiting, abdominal pain, loss of appetite, dark urine, or yellowing of your skin and the whites of your eyes (jaundice). These may not always be related to diabetes medications, but your doctor will need to investigate all possible causes.
- Drug combinations. By combining drugs from different classes, you may be able to control your blood sugar in several different ways. Each class of oral medication can be combined with drugs from any other class. Most doctors prescribe two drugs in combination, although sometimes three drugs may be prescribed. Newer medications, such as Glucovance, which contains both glyburide and metformin, combine different oral drugs in a single tablet.
Nursing Intervention
- Advice patient about the importance of an individualized meal plan in meeting weekly weight loss goals and assist with compliance.
- Assess patients for cognitive or sensory impairments, which may interfere with the ability to accurately administer insulin.
- Demonstrate and explain thoroughly the procedure for insulin self-injection. Help patient to achieve mastery of technique by taking step by step approach.
- Review dosage and time of injections in relation to meals, activity, and bedtime based on patients individualized insulin regimen.
- Instruct patient in the importance of accuracy of insulin preparation and meal timing to avoid hypoglycemia.
- Explain the importance of exercise in maintaining or reducing weight.
- Advise patient to assess blood glucose level before strenuous activity and to eat carbohydrate snack before exercising to avoid hypoglycemia.
- Assess feet and legs for skin temperature, sensation, soft tissues injuries, corns, calluses, dryness, hair distribution, pulses and deep tendon reflexes.
- Maintain skin integrity by protecting feet from breakdown.
- Advice patient who smokes to stop smoking or reduce if possible, to reduce vasoconstriction and enhance peripheral flow.
DOCUMENTATION GUIDELINES
- Results of urine and blood tests for glucose
- Physical findings: Visual problems, skin problems or lesions, changes in sensation or circulation to the extremities
- Patient teaching, return demonstrations, patient’s understanding of teaching
- Response to insulin
DISCHARGE AND HOME HEALTHCARE GUIDELINES
- Diet. Explain how to calculate the American Diabetic Association exchange list to develop a satisfactory diet within the prescribed calories. Emphasize the importance of adjusting diet during illness, growth periods, stress, and pregnancy. Encourage patients to avoid alcohol and refined sugars and to distribute nutrients to maintain a balanced blood sugar throughout the 24-hour period.
- Insulin. Patients need to understand the type of insulin prescribed. Instructions should include onset, peak, and duration of action. Stress proper timing of meals and planning snacks for the time when insulin is at its peak, and recommend an evening snack for those on long-acting insulins. Reinforce that patients cannot miss a dosage and there may be a need for increasing dosages during times of stress or illness. Teaching regarding the proper preparation of insulin, how to administer, and the importance of rotating sites is necessary.
- Urine and Blood Testing. Teach patients the appropriate technique for testing blood and urine and how to interpret the results. Patients need to know when to notify the physician and increase testing during times of illness.
- Skin Care. Stress the importance of close attention to even minor skin injuries. Emphasize foot care, including the importance of properly fitting shoes with clean, nonconstricting socks; daily washing and thorough drying of the feet; and inspection of the toes, with special attention paid to the areas between the toes. Encourage the patient to contact a podiatrist as needed. Because of sensory loss in the lower extremities, teach the patient to test the bath water to prevent skin trauma from water that is too hot and to avoid using heating pads.
- Circulation. Because of the atherosclerotic changes that occur with DM, encourage patients to stop smoking. In addition, teach patients to avoid crossing their legs when sitting and to begin a regular exercise program.
- http://en.wikipedia.org/wiki/Diabetes_mellitus
- http://www.who.int/topics/diabetes_mellitus/en/
- http://www.nurseslearning.com/courses/nrp/NRP1605/course/section2/index.htm
- http://nursingcrib.com/case-study/diabetes-mellitus-case-study/
- http://en.wikipedia.org/wiki/File:Main_symptoms_of_diabetes.png
- Disease and Disorder a Nursing Therapeutic Manual 2007
- http://jalanhealthcare.com/images/diabetes-type1.jpg
- http://jalanhealthcare.com/images/diabetes-type2.jpg
Exam
Nursing Care Plan
Nursing Diagnosis
- Risk for Infection
Risk factors may include
- High glucose levels, decreased leukocyte function, alterations in circulation
- Preexisting respiratory infection, or UTI
Possibly evidenced by
- [Not applicable for risk diagnosis. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.]
Desired Outcomes
- Identify interventions to prevent/reduce risk of infection.
- Demonstrate techniques, lifestyle changes to prevent development of infection.
Nursing Interventions
- Observe for the signs of infection and inflammation: fever, flushed appearance, wound drainage, purulent sputum, cloudy urine.
- Rationale: Patients with DM may be admitted with infection, which could have precipitated the ketoacidotic state. They may also develop nosocomial infection.
- Teach and promote good hand hygiene.
- Rationale: Reduces risk of cross-contamination.
- Maintain asepsis during IV insertion, administration of medications, and providing wound or site care. Rotate IV sites as indicated.
- Rationale: Increased glucose in the blood creates an excellent medium for bacteria to thrive.
- Provide catheter or perineal care. Teach female patients to clean from front to back after elimination.
- Rationale: Minimizes risk of UTI. Comatose patient may be at particular risk if urinary retention occurred before hospitalization. Note: Elderly female diabetic patients are especially prone to urinary tract and/or vaginal yeast infections.
- Provide meticulous skin care: gently massage bony areas, keep skin dry. Keep linens dry and wrinkle-free.
- Rationale: Peripheral circulation may be ineffective or impaired, placing the patient at increased risk for skin breakdown and infection.
- Auscultate breath sounds.
- Rationale: Rhonchi may indicate accumulation of secretions possibly related to pneumonia or bronchitis. Crackles may results from pulmonary congestion or edema from rapid fluid replacement or heart failure.
- Place in semi-Fowler’s position.
- Rationale: Facilitates lung expansion; reduces risk of aspiration
- Reposition and encourage coughing or deep breathing if patient is alert and cooperative. Otherwise, suction airway using sterile technique as needed.
- Rationale: Aids in ventilating all lung areas and mobilizing secretions. Prevents stasis of secretions with increased risk of infection.
- Provide tissues and trash bag in a convenient location for sputum and other secretions. Instruct patient in proper handling of secretions.
- Rationale: To minimizes spread of infection.
- Encourage and assist with oral hygiene.
- Rationale: Reduces risk of oral/gum disease.
- Encourage adequate dietary and fluid intake (approximately 3000 mL/day if not contraindicated by cardiac or renal dysfunction), including 8 oz of cranberry juice per day as appropriate.
- Rationale: Decreases susceptibility to infection. Increased urinary flow prevents stasis and aids in maintaining urine pH/acidity, reducing bacteria growth and flushing organisms out of system. Note: Use of cranberry juice can help prevent bacteria from adhering to the bladder wall, reducing the risk of recurrent UTI.
- Administer antibiotics as appropriate.
- Rationale: Early treatment may help prevent sepsis.
Nursing Diagnosis
- Risk for Disturbed Sensory Perception
Risk factors may include
- Endogenous chemical alteration: glucose/insulin and/or electrolyte imbalance
Possibly evidenced by
- [Not applicable for risk diagnosis. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.]
Desired Outcomes
- Maintain usual level of mentation.
- Recognize and compensate for existing sensory impairments.
Nursing Interventions
- Monitor vital signs and mental status.
- Rationale: To provide baseline from which to compare abnormal findings.
- Call the patient by name, reorient as needed to place, person, and time. Give short explanations, speak slowly and enunciate clearly.
- Rationale: Decreases confusion and helps maintain contact with reality.
- Schedule and cluster nursing time and interventions.
- Rationale: To provide uninterrupted rest periods and promote restful sleep, minimize fatigue and improve cognition.
- Keep patient’s routine as consistent as possible. Encourage participation in activities of daily living (ADLs) as able.
- Rationale: Helps keep patient in touch with reality and maintain orientation to the environment.
- Protect patient from injury by avoiding or limiting the use of restraints as necessary when LOC is impaired. Place bed in low position and pad bed rails if patient is prone to seizures.
- Rationale: Disoriented patients are prone to injury, especially at night, and precautions need to be taken as indicated. Seizure precautions need to be taken as appropriate to prevent physical injury, aspiration, and falls.
- Evaluate visual acuity as indicated.
- Rationale: Retinal edema or detachment, hemorrhage, presence of cataracts or temporary paralysis of extraocular muscles may impair vision, requiring corrective therapy and/or supportive care.
- Observe and investigate reports of hyperesthesia, pain, or sensory loss in the feet or legs. Investigate and look for ulcers, reddened areas, pressure points, loss of pedal pulses.
- Rationale: Peripheral neuropathies may result in severe discomfort, lack of or distortion of tactile sensation, potentiating risk of dermal injury and impaired balance.
- Provide bed cradle. Keep hands and feet warm, avoiding exposure to cool drafts and/or hot water or use of heating pad.
- Rationale: Reduces discomfort and potential for dermal injury.
- Assist patient with ambulation or position changes.
- Rationale: Promotes patient safety, especially when sense of balance is affected.
- Monitor laboratory values: blood glucose, serum osmolality, Hb/Hct, BUN/Cr.
- Rationale: Imbalances can impair mentation. Note: If fluid is replaced too quickly, excess water may enter brain cells and cause alteration in the level of consciousness (water intoxication).
- Carry out prescribed regimen for correcting DKA as indicated.
- Rationale: Alteration in thought processes or potential for seizure activity is usually alleviated once hyperosmolar state is corrected.
Nursing Diagnosis
- Powerlessness
May be related to
- Long-term/progressive illness that is not curable
- Dependence on others
Possibly evidenced by
- Reluctance to express true feelings; expressions of having no control/influence over situation
- Apathy, withdrawal, anger
- Does not monitor progress, nonparticipation in care/decision making
- Depression over physical deterioration/complications despite patient cooperation with regimen
Desired Outcomes
- Acknowledge feelings of helplessness.
- Identify healthy ways to deal with feelings.
- Assist in planning own care and independently take responsibility for self-care activities.
Nursing Interventions
- Encourage patient and/or SO to express feelings about hospitalization and disease in general.
- Rationale: Identifies concerns and facilitates problem solving.
- Acknowledge normality of feelings.
- Rationale: Recognition that reactions are normal can help patient problem-solve and seek help as needed. Diabetic control is a full-time job that serves as a constant reminder of both presence of disease and threat to patient’s health.
- Assess how patient has handled problems in the past. Identify locus of control.
- Rationale: Knowledge of individual’s style helps determine needs for treatment goals. Patient whose locus of control is internal usually looks at ways to gain control over own treatment program. Patient who operates with an external locus of control wants to be cared for by others and may project blame for circumstances onto external factors.
- Provide opportunity for SO to express concerns and discuss ways in which he or she can be helpful to patient
- Rationale: Enhances sense of being involved and gives SO a chance to problem-solve solutions to help patient prevent recurrence.
- Ascertain expectations and/or goals of patient and SO.
- Rationale: Unrealistic expectations or pressure from others or self may result in feelings of frustration and loss of control. These can impair coping abilities.
- Determine whether a change in relationship with SO has occurred.
- Rationale: Constant energy and thought required for diabetic control often shifts the focus of a relationship. Development of psychological concerns affecting self-concept may add further stress.
- Encourage patient to make decisions related to care: ambulation, schedule for activities, and so forth.
- Rationale: Communicates to patient that some control can be exercised over care.
- Support participation in self-care and give positive feedback for efforts.
- Rationale: Promotes feeling of control over situation.
Nursing Diagnosis
- Imbalanced Nutrition: Less Than Body Requirements
May be related to
- Insulin deficiency (decreased uptake and utilization of glucose by the tissues, resulting in increased protein/fat metabolism)
- Decreased oral intake: anorexia, nausea, gastric fullness, abdominal pain; altered consciousness
- Hypermetabolic state: release of stress hormones (e.g., epinephrine, cortisol, and growth hormone), infectious process
Possibly evidenced by
- Increased urinary output, dilute urine
- Reported inadequate food intake, lack of interest in food
- Recent weight loss; weakness, fatigue, poor muscle tone
- Diarrhea
- Increased ketones (end product of fat metabolism)
Desired Outcomes
- Ingest appropriate amounts of calories/nutrients.
- Display usual energy level.
- Demonstrate stabilized weight or gain toward usual/desired range with normal laboratory values.
Nursing Interventions
- Weigh daily or as ordered.
- Rationale: Weighing serves as an assessment tool to determine the adequacy of nutritional intake.
- Ascertain patient’s dietary program and usual pattern then compare with recent intake.
- Rationale: Identifies deficits and deviations from therapeutic needs.
- Auscultate bowel sounds. Note reports of abdominal pain, bloating, nausea, vomiting of undigested food. Maintain NPO status as indicated.
- Rationale: Hyperglycemia and fluid and electrolyte disturbances can decrease gastric motility and/or function (due to distention or ileus) affecting choice of interventions. Note: Chronic difficulties with decreased gastric emptying time and poor intestinal motility may suggest autonomic neuropathies affecting the GI tract and requiring symptomatic treatment.
- Provide liquids containing nutrients and electrolytes as soon as patient can tolerate oral fluids then progress to a more solid food as tolerated.
- Rationale: Oral route is preferred when patient is alert and bowel function is restored.
- Identify food preferences, including ethnic and cultural needs.
- Rationale: If patient’s food preferences can be incorporated into the meal plan, cooperation with dietary requirements may be facilitated after discharge.
- Include SO in meal planning as indicated.
- Rationale: To promote sense of involvement and provide information to the SO to understand the nutritional needs of the patient. Note: Various methods available or dietary planning include exchange list, point system, glycemic index, or pre selected menus.
- Observe for signs of hypoglycemia: changes in LOC, cold and clammy skin, rapid pulse, hunger, irritability, anxiety, headache, lightheadedness, shakiness.
- Rationale: Hypoglycemia can occur once blood glucose level is reduced and carbohydrate metabolism resumes and insulin is being given. If the patient is comatose, hypoglycemia may occur without notable change in LOC. This potentially life-threatening emergency should be assessed and treated quickly per protocol. Note: Type 1 diabetics of long standing may not display usual signs of hypoglycemia because normal response to low blood sugar may be diminished.
- Perform fingerstick glucose testing.
- Rationale: Beside analysis of serum glucose is more accurate than monitoring urine sugar. Urine glucose is not sensitive enough to detect fluctuations in serum levels and can be affected by patient’s individual renal threshold or the presence of urinary retention. Note: Normal levels for fingerstick glucose testing may vary depending on how much the patient ate during his last meal. In general: 80–120 mg/dL (4.4–6.6 mmol/L) before meals or when waking up; 100–140 mg/dL (5.5–7.7 mmol/L) at bedtime.
- Administer regular insulin by intermittent or continuous IV method: IV bolus followed by a continuous drip via pump of approximately 5–10 U/hr so that glucose is reduced by 50 mg/dL/hr.
- Rationale: Regular insulin has a rapid onset and thus quickly helps move glucose into cells. The IV route is the initial route of choice because absorption from subcutaneous tissues may be erratic. Many believe the continuous method is the optimal way to facilitate transition to carbohydrate metabolism and reduce incidence of hypoglycemia.
- Administer glucose solutions: dextrose and half-normal saline.
- Rationale: Glucose solutions may be added after insulin and fluids have brought the blood glucose to approximately 400 mg/dL. As carbohydrate metabolism approaches normal, care must be taken to avoid hypoglycemia.
- Provide diet of approximately 60% carbohydrates, 20% proteins, 20% fats in designated number of meals and snacks.
- Rationale: Complex carbohydrates (apples, broccoli, peas, dried beads, carrots, peas, oats) decrease glucose levels/insulin needs, reduce serum cholesterol levels, and promote satiation. Food intake is scheduled according to specific insulin characteristics and individual patient response. Note: A snack at bedtime of complex carbohydrates is especially important (if insulin is given in divided doses) to prevent hypoglycemia during sleep and potential Somogyi response.
- Administer other medications as indicated: metoclopramide (Reglan); tetracycline.
- Rationale: May be useful in treating symptoms related to autonomic neuropathies affecting GI tract, thus enhancing oral intake and absorption of nutrients.
Nursing Diagnosis
- Deficient Fluid Volume
May be related to
- Osmotic diuresis (from hyperglycemia)
- Excessive gastric losses: diarrhea, vomiting
- Restricted intake: nausea, confusion
Possibly evidenced by
- [Not applicable for risk diagnosis. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.]
Possibly evidenced by
- Increased urinary output, dilute urine
- Weakness; thirst; sudden weight loss
- Dry skin/mucous membranes, poor skin turgor
- Hypotension, tachycardia, delayed capillary refill
Desired Outcomes
- Demonstrate adequate hydration as evidenced by stable vital signs, palpable peripheral pulses, good skin turgor and capillary refill, individually appropriate urinary output, and electrolyte levels within normal range.
Nursing Interventions
- Assess patient’s history related to duration or intensity of symptoms such as vomiting, excessive urination.
- Rationale: Assists in estimation of total volume depletion. Symptoms may have been present for varying amounts of time (hours to days). Presence of infectious process results in fever and hypermetabolic state, increasing insensible fluid losses.
Monitor vital signs:
- Note orthostatic BP changes.
- Rationale: Hypovolemia may be manifested by hypotension and tachycardia. Estimates of severity of hypovolemia may be made when patient’s systolic BP drops more than 10 mmHg from a recumbent to a sitting then a standing position. Note: Cardiac neuropathy may block reflexes that normally increase heart rate.
- Respiratory pattern: Kussmaul’s respirations, acetone breath.
- Rationale: Lungs remove carbonic acid through respirations, producing a compensatory respiratory alkalosis for ketoacidosis. Acetone breath is due to breakdown of acetoacetic acid and should diminish as ketosis is corrected. Correction of hyperglycemia and acidosis will cause the respiratory rate and pattern to approach normal.
- Respiratory rate and quality, use of accessory muscles, periods of apnea, and appearance of cyanosis.
- Rationale: In contrast, increased work of breathing, shallow, rapid respirations, and presence of cyanosis may indicate respiratory fatigue and/or that patient is losing ability to compensate for acidosis.
- Temperature, skin color, moisture, and turgor.
- Rationale: Although fever, chills, and diaphoresis are common with infectious process, fever with flushed, dry skin and decreased skin turgor may reflect dehydration.
- Assess peripheral pulses, capillary refill, and mucous membranes.
- Rationale: Indicators of level of hydration, adequacy of circulating volume.
- Monitor I&O and note urine specific gravity.
- Rationale: Provides ongoing estimate of volume replacement needs, kidney function, and effectiveness of therapy.
- Weigh daily.
- Rationale: Provides the best assessment of current fluid status and adequacy of fluid replacement.
- Maintain fluid intake of at least 2500 mL/day within cardiac tolerance when oral intake is resumed.
- Rationale: Maintains hydration and circulating volume.
- Promote comfortable environment. Cover patient with light sheets.
- Rationale: Avoids overheating, which could promote further fluid loss.
- Investigate changes in mentation and LOC.
- Rationale: Changes in mentation can be due to abnormally high or low glucose, electrolyte abnormalities, acidosis, decreased cerebral perfusion, or developing hypoxia. Regardless of the cause, impaired consciousness can predispose patient to aspiration.
- Insert and maintain indwelling urinary catheter.
- Rationale: Provides for accurate ongoing measurement of urinary output, especially if autonomic neuropathies result in neurogenic bladder (urinary retention/overflow incontinence). May be removed when patient is stable to reduce risk of infection.
Nursing Diagnosis
- Fatigue
May be related to
- Decreased metabolic energy production
- Altered body chemistry: insufficient insulin
- Increased energy demands: hypermetabolic state/infection
Possibly evidenced by
- Overwhelming lack of energy, inability to maintain usual routines, decreased performance, accident-prone
- Impaired ability to concentrate, listlessness, disinterest in surroundings
Desired Outcomes
- Verbalize increase in energy level.
- Display improved ability to participate in desired activities.
Nursing Interventions
- Discuss with patient the need for activity. Plan schedule with patient and identify activities that lead to fatigue.
- Rationale: Education may provide motivation to increase activity level even though patient may feel too weak initially.
- Alternate activity with periods of rest and uninterrupted sleep.
- Rationale: To prevent excessive fatigue.
- Monitor pulse, respiratory rate, and BP before and after activity.
- Rationale: Indicates physiological levels of tolerance.
- Discuss ways of conserving energy while bathing, transferring, and so on.
- Rationale: Patient will be able to accomplish more with a decreased expenditure of energy.
- Increase patient participation in ADLs as tolerated.
- Rationale: Increases confidence level, self-esteem and tolerance level.
Nursing diagnosis
- Deficient Fluid Volume related to intracellular dehydration secondary to diabetes mellitus
Possibly evidenced by
- Elevated temperature
- Increased urine output
- Sweating
- Thirst
- Exhaustion
- Weight loss
- Dry skin and/or mucous membrane
Desired outcomes
- Patient will verbalize understanding of causative factors and purpose of individual therapeutic interventions and medications.
- Patient will improve or maintain fluid volume at a functional level as evidenced by individual good skin turgor, moist mucous membrane, and stable vital signs.
Nursing Interventions
- Establish rapport
- Rationale: Friendly and trusting relationship with patient and to be able to understand each other’s concern.
- Take and record vital signs.
- Rationale: To obtain baseline data.
- Monitor the temperature.
- Rationale: To monitor changes in temperature.
- Assess skin turgor and mucous membranes for signs of dehydration.
- Rationale: Dry mucous membranes are signs of dehydration.
- Monitor intake and output
- Rationale: To assess for signs of dehydration.
- Encourage patient to increase fluid intake as tolerated.
- Rationale: To replace fluid loss and prevent dehydration.
- Administer IVF as ordered.
- Rationale: To replace lost electrolytes and fluids.
Nursing Diagnosis
- Imbalanced Nutrition: less than body requirement r/t insulin deficiency
Possibly evidenced by
- Poor muscle tone
- Generalized weakness
- Increased thirst
- Increased urination
- Polyphagia
- Loss of weight
Desired outcomes
- Patient will verbalize understanding of causative factors when known and necessary interventions are identified for diabetic client.
- Patient will demonstrate improvement of weight and nutrition towards goal.
Nursing Interventions
- Ascertain understanding of individual nutritional needs.
- Rationale: To determine what information to be provided to client or SO.
- Discuss eating habits and encourage diabetic diet (balanced diet) as prescribed by the doctor.
- Rationale: To achieve health needs of the patient with the proper food diet for his condition.
- Document actual weight, do not estimate. Note total daily intake including patterns and time of eating.
- Rationale: Patients may be unaware of their actual weight or weight loss due to estimation of weight.
- Consult dietician and/or physician for further assessment and recommendation regarding food preferences and nutritional support.
- Rationale: To reveal changes that should be made in the client’s dietary intake. For greater understanding and further assessment of specific foods.
Nursing Diagnosis
- Risk for Infection
Risk factors
- Chronic hyperglycemia
- Neurogenic bladder
- Peripheral vascular disease
Possibly evidenced by
- [Not applicable for risk diagnosis. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.]
Desired outcomes
- Patient will be free of infections as evidenced by normothermia, negative cultures, and WBC within normal levels.
Nursing Interventions
- Assess temperature every four (4) hours. Notify physician if fever occurs.
- Rationale: Fever is a sign of an infection Infection is the most common cause of diabetic ketoacidosis (DKA).
- Monitor for signs of infection (e.g., fever, rhonchi, dyspnea, and/or cough).
- Rationale: These are indicators of pneumonia which is common among patients with DM.
- Assess for dysuria, tachycardia, diaphoresis, nausea, vomiting, and abdominal pain.
- Rationale: These are indicators of UTI. Neurogenic bladder predisposes to UTI.
- Assess for erythema, swelling, and purulent drainage at IV sites.
- Rationale: These are signs of IV catheter infections.
Nursing Diagnosis
- Risk for Impaired Skin Integrity
Risk factors
- Decreased circulation and sensation caused by peripheral neuropathy and arterial obstruction.
Possibly evidenced by
- [Not applicable for risk diagnosis. A risk diagnosis is not evidenced by signs and symptoms, as the problem has not occurred and nursing interventions are directed at prevention.]
Desired outcomes
- Patient’s skin on legs and feet remains intact while the patient is hospitalized.
- Patient will demonstrate proper foot care.
Nursing Interventions
- Assess integrity of the skin. Assess knee and deep tendon reflexes and proprioception.
- Rationale: These are assessments for neuropathy. Skin on lower extremity pressure points is at great risk for ulceration.
- Use foot cradle on the bed. Use space boots on ulcerated heels, elbow protectors, and pressure-relief mattresses.
- Rationale: To prevent pressure on pressure-sensitive points.
- Wash feet daily with mild soap and warm water. Check water temperature before immersing feet in the water.
- Rationale: Decreased sensation increases the risk for burns.
- Inspect feet daily for erythema or trauma.
- Rationale: These are signs that the skin needs preventive care.
- Change socks or stockings daily. Encourage the patient to wear white cotton socks.
- Rationale: To prevent infection from moisture. White fabric enables easy visualization of blood or exudates.
- Use gentle moisturizers on the feet.
- Rationale: Moisturizers soften and lubricate dry skin, preventing skin cracking.
- Cut toenails straight across after softening toenails with a bath.
- Rationale: This action prevents ingrown toenails, which could cause infection.
- The patient should not walk barefoot.
- Rationale: This is a high risk for trauma and may result in ulceration and infection.


