Definition
- Excision of painful distended veins of the anus and rectum.
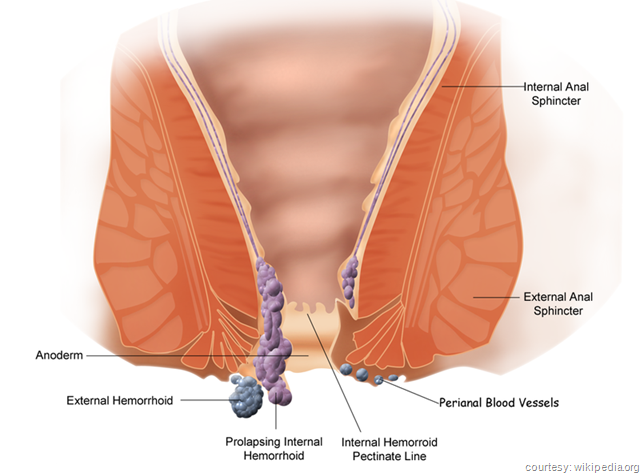
- Hemorrhoids are classified as internal or external, depending on their location. Hemorrhoids are generally associated with local anal problems such as anal ulcers and fistulas, or they may accompany pregnancy. Anesthesia may be regional, local, or general.

Position
- Lithotomy, modified lateral (Sims), or jack knife.
Skin Preparation
- The buttocks is taped apart with wide adhesive tape on each side of the anus, attaching the other end to the table frame. Only a minimal prep is usually performed.
Packs/ Drapes
- Laparotomy pack (jackknife or lateral sims position)
- Lithotomy pack (lithotomy position)
Instrumentation
- Minor tray
- Rectal tray with dilators and rectractor
- Sigmoidoscopy instrument (optional)
Supplies/ Equipment
- Stirrups
- Pillows or roll for positioning
- Suction
- Blades – (1) #10, (1) #15
- Minor basin set
- Needle counter
- Hemostatic agent
- Lubricant
- Pressure dressing
- Laser (optional)
Procedure Overview
- Before beginning the surgical procedure, a sigmoidoscopy may be performed, followed by gentle dilation of the rectum.
- The hemorrhoid is grasped with a Penington, Allis, or Kocher clamp.
- The proximal portion of the hemorrhoid is excised by scalpel, cautery, or laser. Is the anus is stemotic, the distal internal sphincter may be incised.
- A mucous membrane flap and/ or skin flaps may be used to cover the denuded areas.
- Bleeders are controlled with ligature ties (3-0 Dexon/ chromic) or by cautery.
- Care is taken not to excise too much skin, anoderm, or mucous membrane and to avoid injury to the sphincter mechanism.
Perioperative Nursing Considerations
- Be prepared to perform a sigmoidoscopy prior to the procedure.
- When electrosurgical unit is used, apply the ground pad after the patient has been placed in the lithotomy position.
- Protect the skin under the adhesive tape with tincture of benzoin.
- Should laser be used, all safety precautions must be in place prior to the patient’s entry into the procedure room.
")
