Notes
Definition
- The term inflammatory bowel disease (IBD) is used to identify two chronic inflammatory GI disorders; regional enteritis (i.e. Crohn’s disease) and ulcerative colitis.
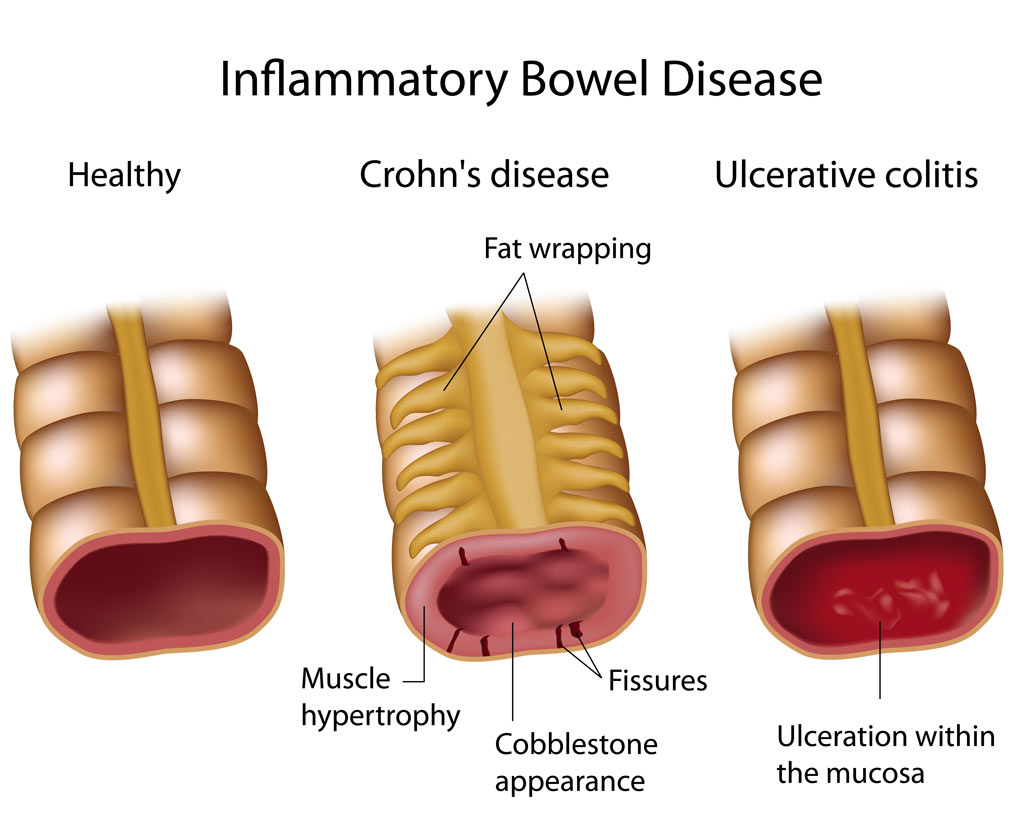
image courtesy of : http://childrensgimd.com/
Risk Factors
- Food additivies
- Tobacco
- Radiation exposure
- Immunologic influences
- Hereditary
Pathophysiology
Regional enteritis
- Is a subacute and chronic inflammation that extends through layers of the bowel walls from the intestinal mucosa. Fistula, fissures, and abscesses extend into the peritoneum, but segments of normal intestinal tissue occur between the inflammations.
Ulcerative colitis
- Is an inflammatory disease of the submucosal layer of the colon and rectum characterized by continuously occurring ulcerations and shedding of intestinal epithelium. Fat deposits and muscular hypertrophy result in a narrow, short, and thickened bowel.
Assessment/Clinical Manifestations/Signs and Symptoms
Regional enteritis
- Abdominal tenderness and pain, typically colicky and increased after meals
- Diarrhea, flatulence, and steatorrhea
- Fever, malaise, and anorexia
- Signs of nutritional deficits
- Perianal fistulas and abscesses
- Usually occurs in ileum and ascending colon
Ulcerative colitis
- Severe diarrhea containing pus, blood and mucosa
- Abdominal cramping and tenderness, fever
- Anorexia and weight loss
- Usually occurs in the descending colon and rectum
Laboratory and diagnostic study findings:
Regional enteritis
- Barium study of the upper GI tract, the most conclusive diagnostic test, reveals the classic “string sign” on a X-ray study of the terminal ileum indicating constriction of a segment of intestine.
- Barium enema shows ulceration and “cobblestone” appearance because of fissures surrounded by submucosal edema.
- Colonoscopy visualizes distinct ulceration separated by relatively normal mucosa in the ileum and ascending colon.
- Computed tomography scan shows bowel wall thickening and fistula tracts.
Ulcerative colitis
- Barium enema shows mucosal irregularities, shortening of the bowel, and dilation of bowel loops
- Colonoscopy shows friable mucosa with pseudopolyps or ulcers in the descending colon and sigmoid colon.
- Stool analysis is positive for blood. Entemoeba histolytica, which causes dysentery, must be ruled out.
Medical Management
- Surgery may include total colectomy with ileostomy; segmental colectomy with anastomosis, subtotal colectomy; total colectomy with continent ilestomy, and total colectomy with ileoanal anastomosis.
Nursing Management
Enhance nutritional status.
- Promote nursing care of the client who is receiving nothing by mouth, receiving oral fluids, or on total parenteral nutrition during an acute exacerbation.
- Assess for fluid and electrolyte imbalance. Administer IV fluids and electrolytes as indicated.
- Encourage a low-residue, high-protein, high-calorie diet with supplemental vitamin therapy and iron replacement.
- Implement measures to treat diarrhea or constipation.
Minimize pain.
- Address and mediate the client’s pain. Promote intermittent rest periods and bed rest when the client has acute exacerbations.
Promote client and family teaching.
- Encourage the client to seek psychotherapy to determine the factors that distress the client and how to deal with these factors to preventexacerbations.
Provide client teaching covering:
- The importance of good nutrition and adequate fluid intake
- Stress-management techniques
- Perianal skin care
- The need for follow-up visits to the health care provider
Administer medications, which include antidiarrheals, corticosteroids, antibiotics, antispasmodics, and anticholinergic and opioid analgesics.
Nursing Care Plan
Nursing Diagnosis
- Diarrhea
May be related to
- Inflammation, irritation, or malabsorption of the bowel
- Presence of toxins
- Segmental narrowing of the lumen
Possibly evidenced by
- Increased bowel sounds/peristalsis
- Hyperactive bowel sounds
- Frequent, and often severe, watery stools (acute phase)
- Changes in stool color
- Abdominal pain; urgency (sudden painful need to defecate), cramping
Desired Outcomes
- Report reduction in frequency of stools, return to more normal stool consistency.
- Identify/avoid contributing factors.
Nursing Interventions
- Ascertain onset and pattern of diarrhea
- Rationale: To assess etiology. Chronic diarrhea (caused by irritable bowel syndrome, infectious diseases affecting colon such as IBD).
- Observe and record stool frequency, characteristics, amount, and precipitating factors.
- Rationale: Helps differentiate individual disease and assesses severity of episode.
- Observe for presence of associated factors, such as fever, chills, abdominal pain,cramping, bloody stools, emotional upset, physical exertion and so forth.
- Rationale: To assess causative factors and etiology.
- Promote bedrest, provide bedside commode.
- Rationale: Rest decreases intestinal motility and reduces the metabolic rate when infection or hemorrhage is a complication. Urge to defecate may occur without warning and be uncontrollable, increasing risk of incontinence or falls if facilities are not close at hand.
- Remove stool promptly. Provide room deodorizers.
- Rationale: Reduces noxious odors to avoid undue patient embarrassment.
- Identify and restrict foods and fluids that precipitate diarrhea (vegetables and fruits, whole-grain cereals, condiments, carbonated drinks, milk products).
- Rationale: Avoiding intestinal irritants promote intestinal rest and reduce intestinal workload.
- Restart oral fluid intake gradually. Offer clear liquids hourly; avoid cold fluids.
- Rationale: Provides colon rest by omitting or decreasing the stimulus of foods and fluids. Gradual resumption of liquids may prevent cramping and recurrence of diarrhea; however, cold fluids can increase intestinal motility.
- Provide opportunity to vent frustrations related to disease process.
- Rationale: Presence of disease with unknown cause that is difficult to cure and that may require surgical intervention can lead to stress reactions that may aggravate condition.
- Observe for fever, tachycardia, lethargy, leukocytosis, decreased serum protein, anxiety, and prostration.
- Rationale: May signify that toxic megacolon or perforation and peritonitis are imminent or have occurred, necessitating immediate medical intervention.
Nursing Diagnosis
- Risk for Deficient Fluid Volume
Risk factors may include
- Excessive losses through normal routes (severe frequent diarrhea, vomiting)
- Hypermetabolic state (inflammation, fever)
- Restricted intake (nausea/anorexia)
- Hemoconcentration; altered serum sodium
Desired Outcomes
- Maintain adequate fluid volume as evidenced by moist mucous membranes, good skin turgor, and capillary refill; stable vital signs; balanced I&O with urine of normal concentration/amount.
- Demonstrate behaviors to monitor and correct deficit, as indicated, when condition is chronic.
Nursing Interventions
- Note possible conditions or processes that may lead to deficits such as fluid loss, limited intake, fluid shifts, environmental factor.
- Rationale: To assess causative and precipitating factors. Fluid loss may be an effect of diarrhea or vomiting).
- Monitor I&O. Note number, character, and amount of stools; estimate insensible fluid losses (diaphoresis). Measure urine specific gravity; observe for oliguria.
- Rationale: Provides information about overall fluid balance, renal function, and bowel disease control, as well as guidelines for fluid replacement.
- Assess vital signs (BP, pulse, temperature).
- Rationale: Hypotension (including postural), tachycardia, fever can indicate response of fluid loss.
- Observe for excessively dry skin and mucous membranes, decreased skin turgor, slowed capillary refill.
- Rationale: Indicates excessive fluid loss or resultant dehydration.
- Weigh daily.
- Rationale: Indicator of overall fluid and nutritional status.
- Maintain oral restrictions, bedrest; avoid exertion.
- Rationale: Colon is placed at rest for healing and to decrease intestinal fluid losses.
- Observe for overt bleeding and test stool daily for occult blood.
- Rationale: Inadequate diet and decreased absorption may lead to vitamin K deficiency and defects in coagulation, potentiating risk of hemorrhage.
- Note generalized muscle weakness or cardiac dysrhythmias.
- Rationale: Excessive intestinal loss may lead to electrolyte imbalance, e.g., potassium, which is necessary for proper skeletal and cardiac muscle function. Minor alterations in serum levels can result in profound or life-threatening symptoms.
- Administer parenteral fluids, blood transfusions as indicated.
- Rationale: Maintenance of bowel rest requires alternative fluid replacement to correct losses and anemia. Note: Fluids containing sodium may be restricted in presence of regional enteritis.
- Monitor laboratory studies such as electrolytes (especially potassium, magnesium) and ABGs (acid-base balance).
- Rationale: Determines replacement needs and effectiveness of therapy.
Nursing Diagnosis
- Anxiety [specify level]
May be related to
- Physiological factors/sympathetic stimulation (inflammatory process)
- Threat to self-concept (perceived or actual)
- Threat to/change in health status, socioeconomic status, role functioning, interaction patterns
Possibly evidenced by
- Exacerbation of acute stage of disease
- Increased tension, distress, apprehension
- Expressed concern regarding changes in life
- Somatic complaints
- Focus on self
Desired Outcomes
- Appear relaxed and report anxiety reduced to a manageable level.
- Verbalize awareness of feelings of anxiety and healthy ways to deal with them.
- Identify healthy ways to deal with and express anxiety.
- Use support system effectively.
Nursing Interventions
- Review physiological factors, such as active medical condition; recent or ongoing stressors.
- Rationale: These factors can cause or exacerbate anxiety or anxiety disorders.
- Observe and note behavioral clues (restlessness, irritability, withdrawal, lack of eye contact, demanding behavior).
- Rationale: Indicators of degree of anxiety or stress (patient may feel out of control at home or at work managing personal problems.Stress may develop as a result of physical symptoms of condition and the reaction of others.
- Encourage verbalization of feelings. Provide feedback.
- Rationale: Establishes a therapeutic relationship. Assists patient and SO in identifying problems causing stress. Patient with severe diarrhea may hesitate to ask for help for fear of becoming a burden to the staff.
- Acknowledge that the anxiety and problems are similar to those expressed by others. Active-Listen patient’s concerns.
- Rationale: Validation that feelings are normal can help reduce stress, isolation and belief that “I am the only one.”
- Provide accurate, concrete information about what is being done (reason for bedrest, restriction of oral intake, and procedures).
- Rationale: Involving patient in plan of care provides sense of control and helps decrease anxiety.
- Provide a calm, restful environment.
- Rationale: Removing patient from outside stressors promotes relaxation; helps reduce anxiety.
- Encourage staff and SO to project caring, concerned attitude.
- Rationale: A supportive manner can help patient feel less stressed, allowing energy to be directed toward healing or recovery.
- Help patient identify and initiate positive coping behaviors used in the past.
- Rationale: Successful behaviors can be fostered in dealing with current problems and stress, enhancing patient’s sense of self-control.
- Assist patient to learn new coping mechanisms (stress management techniques, organizational skills).
- Rationale: Learning new ways to cope can be helpful in reducing stress and anxiety, enhancing disease control.
Nursing Diagnosis
- Pain, acute
May be related to
- Hyperperistalsis, prolonged diarrhea, skin/tissue irritation, perirectal excoriation, fissures, fistulas
Possibly evidenced by
- Reports of colicky/cramping abdominal pain/referred pain
- Guarding/distraction behaviors, restlessness
- Facial mask of pain; self-focusing
Desired Outcomes
- Report pain is relieved/controlled.
- Appear relaxed and able to sleep/rest appropriately.
Nursing Interventions
- Encourage patient to report pain.
- Rationale: May try to tolerate pain rather than request analgesics.
- Assess reports of abdominal cramping or pain, noting location, duration, intensity (0–10 scale). Investigate and report changes in pain characteristics
- Rationale: Colicky intermittent pain occurs with Crohn’s disease
- Note nonverbal cues (restlessness, reluctance to move, abdominal guarding, withdrawal, and depression). Investigate discrepancies between verbal and nonverbal cues.
- Rationale: Body language or nonverbal cues may be both physiological and psychological and may be used in conjunction with verbal cues to determine extent and severity of the problem.
- Review factors that aggravate or alleviate pain.
- Rationale: May pinpoint precipitating or aggravating factors (such as stressful events, food intolerance) or identify developing complications.
- Encourage patient to assume position of comfort (knees flexed).
- Rationale: Reduces abdominal tension and promotes sense of control.
- Provide comfort measures (back rub, reposition) and diversional activities.
- Rationale: Promotes relaxation, refocuses attention, and may enhance coping abilities.
- Cleanse rectal area with mild soap and water or wipes after each stool and provide skin care (A&D ointment, Sween ointment, karaya gel, Desitin, petroleum jelly).
- Rationale: Protects skin from bowel acids, preventing excoriation.
- Provide sitz bath as appropriate.
- Rationale: Enhances cleanliness and comfort in the presence of perianal irritation or fissures.
- Observe for ischiorectal and perianal fistulas.
- Rationale: Fistulas may develop from erosion and weakening of intestinal bowel wall.
- Observe and record abdominal distension, increased temperature, decreased BP.
- Rationale: May indicate developing intestinal obstruction from inflammation, edema, and scarring.
- Implement prescribed dietary modifications (commence with liquids and increase to solid foods as tolerated).
- Rationale: Complete bowel rest can reduce pain, cramping.
Nursing Diagnosis
- Ineffective Coping
May be related to
- Multiple stressors, repeated over period of time; situational crisis
- Unpredictable nature of disease process
- Personal vulnerability; inadequate coping method; lack of support systems
- Severe pain
- Lack of sleep, rest
Possibly evidenced by
- Verbalization of inability to cope, discouragement, anxiety
- Preoccupation with physical self, chronic worry, emotional tension, poor self-esteem
- Depression and dependency
Desired Outcomes
- Assess the current situation accurately.
- Identify ineffective coping behaviors and consequences.
- Acknowledge own coping abilities.
- Demonstrate necessary lifestyle changes to limit/prevent recurrent episodes.
Nursing Interventions
- Assess patient’s and SO’s understanding and previous methods of dealing with disease process.
- Rationale: Enables the nurse to deal more realistically with current problems. Anxiety and other problems may have interfered with previous health teaching and patient learning.
- Determine outside stressors (family, relationships, social or work environment).
- Rationale: Stress can alter autonomic nervous response, affecting the immune system and contributing to exacerbation of disease. Even the goal of independence in the dependent patient can be an added stressor.
- Provide opportunity for patient to discuss how illness has affected relationship, including sexual concerns.
- Rationale: Stressors of illness affect all areas of life, and patient may have difficulty coping with feelings of fatigue and pain in relation to relationship and sexual needs.
- Help patient identify individually effective coping skills.
- Rationale: Use of previously successful behaviors can help patient deal with current situation and plan for future.
- Provide emotional support:Active-Listen in a nonjudgmental manner;Maintain nonjudgmental body language when caring for patient;Assign same staff as much as possible.
- Rationale: Aids in communication and understanding patient’s viewpoint. Adds to patient’s feelings of self-worth.Prevents reinforcing patient’s feelings of being a burden, (frequent need to empty bedpan or commode). Provides a more therapeutic environment and lessens the stress of constant adjustments.
- Provide uninterrupted sleep and rest periods.
- Rationale: Exhaustion brought on by the disease tends to magnify problems, interfering with ability to cope.
- Encourage use of stress management skills, (relaxation techniques, visualization, guided imagery, deep-breathing exercises).
- Rationale: Refocuses attention, promotes relaxation, and enhances coping abilities.
- Include patient and SO in team conferences to develop individualized program.
- Rationale: Promotes continuity of care and enables patient and SO to feel a part of the plan, imparting a sense of control and increasing cooperation with therapeutic regimen.
- Administer medications as indicated: antianxiety agents, such as lorazepam (Ativan), alprazolam (Xanax).
- Rationale: Aids in psychological and physical rest. Conserves energy and may strengthen coping abilities.
- Refer to resources as indicated (local support group, social worker, psychiatric clinical nurse specialist, spiritual advisor).
- Rationale: Additional support and counseling can assist patient and SO in dealing with specific stress and problem areas.
Nursing Diagnosis
- Nutrition: imbalanced, less than body requirements
May be related to
- Altered absorption of nutrients
- Hypermetabolic state
- Medically restricted intake; fear that eating may cause diarrhea
Possibly evidenced by
- Weight loss; decreased subcutaneous fat/muscle mass; poor muscle tone
- Hyperactive bowel sounds; steatorrhea
- Pale conjunctiva and mucous membranes
- Aversion to eating
Desired Outcomes
- Demonstrate stable weight or progressive gain toward goal with normalization of laboratory values and absence of signs of malnutrition.
Nursing Interventions
- Weigh daily.
- Rationale: Provides information about dietary needs and effectiveness of therapy.
- Encourage bedrest and limited activity during acute phase of illness.
- Rationale: Decreasing metabolic needs aids in preventing caloric depletion and conserves energy.
- Recommend rest before meals.
- Rationale: Quiets peristalsis and increases available energy for eating.
- Provide oral hygiene.
- Rationale: A clean mouth can enhance the taste of food.
- Serve foods in well-ventilated, pleasant surroundings, with unhurried atmosphere, congenial company.
- Rationale: Pleasant environment aids in reducing stress and is more conducive to eating.
- Avoid or limit foods that might cause or exacerbate abdominal cramping, flatulence (milk products, foods high in fiber or fat, alcohol, caffeinated beverages, chocolate, peppermint, tomatoes, orange juice).
- Rationale: Individual tolerance varies, depending on stage of disease and area of bowel affected.
- Record intake and changes in symptomatology.
- Rationale: Useful in identifying specific deficiencies and determining GI response to foods.
- Promote patient participation in dietary planning as possible.
- Rationale: Provides sense of control for patient and opportunity to select foods desired, which may increase intake.
- Encourage patient to verbalize feelings concerning resumption of diet.
- Rationale: Hesitation to eat may be result of fear that food will cause exacerbation of symptoms.
- Keep patient NPO as indicated.
- Rationale: Resting the bowel decreases peristalsis and diarrhea, limiting malabsorption and loss of nutrients.
- Resume or advance diet as indicated (clear liquids progressing to bland, low residue; then high-protein, high-calorie, caffeine-free, nonspicy, and low-fiber as indicated).
- Rationale: Allows the intestinal tract to readjust to the digestive process. Protein is necessary for tissue healing integrity. Low bulk decreases peristaltic response to meal. Note: Dietary measures depend on patient’s condition (if disease is mild, patient may do well on low-residue, low-fat diet high in protein and calories with lactose restriction). In moderate disease, elemental enteral products may be given to provide nutrition without overstimulating the bowel. Patient with toxic colitis is NPO and placed on parenteral nutrition.
Nursing Diagnosis
- Deficient Knowledge
May be related to
- Information misinterpretation, lack of recall
- Unfamiliarity with resources
Possibly evidenced by
- Questions, request for information, statements of misconceptions
- Inaccurate follow-through of instructions
- Development of preventable complications/exacerbations
Desired Outcomes
- Verbalize understanding of disease processes, possible complications.
- Identify stress situations and specific action(s) to deal with them.
- Verbalize understanding of therapeutic regimen.
- Participate in treatment regimen.
- Initiate necessary lifestyle changes.
Nursing Interventions
- Determine patient’s perception of disease process.
- Rationale: Establishes knowledge base and provides some insight into individual learning needs.
- Review disease process, cause and effect relationship of factors that precipitate symptoms, and identify ways to reduce contributing factors. Encourage questions.
- Rationale: Precipitating or aggravating factors are individual; therefore, patient needs to be aware of what foods, fluids, and lifestyle factors can precipitate symptoms. Accurate knowledge base provides opportunity for patient to make informed decisions and choices about future and control of chronic disease. Although most patients know about their own disease process, they may have outdated information or misconceptions.
- Review medications, purpose, frequency, dosage, and possible side effects.
- Rationale: Promotes understanding and may enhance cooperation with regimen.
- Remind patient to observe for side effects if steroids are given on a long-term basis (ulcers, facial edema, muscle weakness).
- Rationale: Steroids may be used to control inflammation and to effect a remission of the disease; however, drug may lower resistance to infection and cause fluid retention.
- Stress importance of good skin care (proper handwashing techniques and perineal skin care).
- Rationale: Reduces spread of bacteria and risk of skin irritation or breakdown, infection.
- Recommend cessation of smoking.
- Rationale: Can increase intestinal motility, aggravating symptoms.
- Emphasize need for long-term follow-up and periodic reevaluation.
- Rationale: Patients with IBD are at increased risk for colon or rectal cancer, and regular diagnostic evaluations may be required.
- Identify appropriate community resources [Crohn’s and Colitis Foundation of America, (CCFA), United Ostomy Association, home healthcare providers or visiting nurse services, dietitian, and social services].
- Rationale: Patient may benefit from the services of these agencies in coping with chronicity of the disease and evaluating treatment options.

