Notes
Description
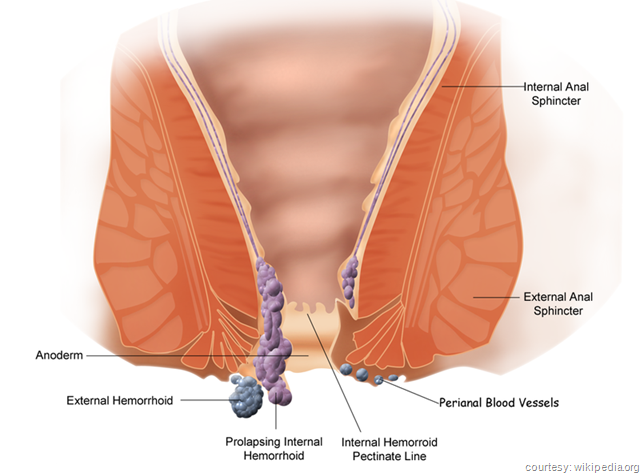
- Hemorrhoids are vascular masses that protrude into the lumen of the lower rectum or perianal area.
- They result when increased intra-abdominal pressure causes engorgement in the vascular tissue lining the anal canal.
- Loosening of vessels from surrounding connective tissue occurs with protrusion or prolapse into the anal canal.
- There are two main types of hemorrhoids: external hemorrhoids appear outside the external sphincter, and internal hemorrhoids appear above the internal sphincter.
- When blood within the hemorrhoids becomes clotted because of obstruction, the hemorrhoids are referred to as being thrombosed.
- Predisposing factors include pregnancy, prolonged sitting or standing, straining stool, chronic constipation or diarrhea, anal infection, rectal surgery or episiotomy, genetic predisposition, alcoholism, portal hypertension (cirrhosis), coughing, sneezing, or vomiting, loss of muscle tone attributable to old age, and anal intercourse.
- Complications include hemorrhage, anemia, incontinence of stool, and strangulation.
- Hemorrhoids are the most common of a variety of anorectal disorders.
Causes/Risk Factors
Modifiable
- Some factors that are associated with hemorrhoids are occupations that require prolonged sitting or standing; heart failure; anorectal infections; anal intercourse; alcoholism; pregnancy; colorectal cancer; and hepatic disease such as cirrhosis, amoebic abscesses, or hepatitis.
- Straining because of constipation, diarrhea, coughing, sneezing, or vomiting and loss of muscle tone because of aging, rectal surgery, or episiotomy can also cause hemorrhoids.
Assessment
- Pain (more so with external hemorrhoids), sensation of incomplete fecal evacuation, constipation, and anal itching. Sudden rectal pain may occur if external hemorrhoids are thrombosed.
- Bleeding may occur during defecation; bright red blood on stool caused by injury of mucosa covering hemorrhoid.
- Visible and palpable masses at anal area.
Diagnostic Evaluation
- External examination with anoscope or proctoscope shows single or multiple hemorrhoids.
- Barium edema or colonoscopy rules out more serious colonic lesions causing rectal bleeding such as polyps.
Primary Nursing Diagnosis
- Pain (acute or chronic) related to rectal swelling and prolapse
Therapeutic Intervention / Medical Management
- High-fiber diet to keep stools soft.
- Warm sitz baths to ease pain and combat swelling.
- Reduction of prolapsed external hemorrhoid manually.
Surgical Interventions:
- Injection of sclerosing solutions to produce scar tissue and decrease prolapse is an office procedure.
- Cryodestruction (freezing) of hemorrhoids is an office procedure.
- Surgery may be indicated in presence of prolonged bleeding, disabling pain, intolerable itching, and general unrelieved discomfort.
Pharmacologic Intervention
- Stool softeners to keep stools soft and relieve symptoms.
- Topical creams, suppositories or other preparation such as Anusol, Preparation H, and witch-hazel compresses to reduce itching and provide comfort.
- Oral analgesics may be needed.
Nursing Intervention
- After thrombosis or surgery, assist with frequent repositioning using pillow support for comfort.
- Provide analgesics, warm sitz baths, or warm compresses to reduce pain and inflammation.
- Apply witch-hazel dressing to perianal area or anal creams or suppositories, if ordered, to relieve discomfort.
- Observe anal area postoperatively for drainage and bleeding.
- Administer stool softener or laxative to assist with bowel movements soon after surgery, to reduce risk of stricture.
- Teach anal hygiene and measures to control moisture to prevent itching.
- Encourage the patient to exercise regularly, follow a high fiber diet, and have an adequate fluid intake (8 to 10 glasses per day) to avoid straining and constipation, which predisposes to hemorrhoid formation.
- Discourage regular use of laxatives; firm, soft stools dilate the anal canal and decrease stricture formation after surgery.
- Tell patient to expect a foul-smelling discharge for 7 to 10 days after cryodestruction.
- Determine the patient’s normal bowel habits and identify predisposing factors to educate patient about preventing recurrence of symptoms.
Documentation Guidelines
- Physical findings:Rectal examination,urinary retention,bleeding,and mucous drainage
- Wound healing:Drainage,color,swelling
- Pain management:Pain (location,duration,frequency),response to interventions
- Postoperative bowel movements:Tolerance for first bowel movement
Discharge and Home Healthcare Guidelines
Teach the patient the importance of a high-fiber diet, increased fluid intake, mild exercise, and regular bowel movements. Be sure the patient schedules a follow-up visit to the physician. Teach the patient which analgesic applications for local pain may be used. If the patient has had surgery, teach her or him to recognize signs of urinary retention, such as bladder distension and hemorrhage,and to contact the physician at their appearance.
Sources:
Nursingcrib.com
Marilyn Sawyer Sommers, RN, PhD, FAAN , Susan A. Johnson, RN, PhD, Theresa A. Beery, PhD, RN , DISEASES AND DISORDERS A Nursing
Therapeutics Manual, 2007 3rd ed
Exam
Nursing Care Plan
Nursing Care Plan for Hemorrhoids
Nursing Diagnosis
Impaired Tissue Integrity
May be related to
- Hemorrhoidal surgery and procedures
- Alteration in activity
- Changes in mobility
- Aging process
- Loss of elasticity of skin
Possibly evidenced by
- Disruption of skin tissue from incisional sites
- Destruction of skin layers
- Thrombosed hemorrhoids
- Internal prolapsed hemorrhoids
- Pain
- Swelling
- Drainage
Desired Outcomes
- Patient will have intact skin with no signs or symptoms of rectal prolapse or bleeding.
- Hemorrhoids will be reduced or removed.
- Patient will exhibit no evidence of thrombosed hemorrhoids or rectal bleeding.
- Patient will have normal CBC with no noted anemias.
- Patient will be able to accurately verbalize understanding of causes of hemorrhoids, methods of preventing the worsening of hemorrhoids, and comfort measures to employ.
- Swollen hemorrhoids will be reduced in size, with no pain evoked.
- Patient will be able to tolerate procedures to diagnose problem and to treat hemorrhoids without the presence of any complication.
Nursing Interventions
- Assess patient for presence of hemorrhoids, discomfort or pain associated with hemorrhoids, diet, fluid intake, and presence of constipation.
- Rationale: Provides baseline information as to type of hemorrhoids (external or internal), degree of venous thrombosis, presence of complications, including bleeding, and risk factors that preclude patient to hemorrhoids to enable initiation of care plan appropriate for patient.
- Administer topical medication as ordered.
- Rationale: Reduces swelling, pain, and/or itching in order to make patient more comfortable.
- Provide “donut cushion” for patient to sit on if needed.
- Rationale: Hemorrhoids are exquisitely painful and patient may not be able to sit in chair and apply pressure to delicate tissues. Donut cushions can help remove pressure from the hemorrhoid; caution on the occurrence of pressure areas.
- Administer stool softeners as ordered.
- Rationale:Helps prevent straining and increases pressure that may cause clotted vessels to rupture or cause further hemorrhoids to develop. Helps relieve pain by avoiding passage of hard fecal material.
- Assist with procedures for treatment of hemorrhoids.
- Rationale:
- Sclerotherapy may be used if problem is detected early, it involves injection of quinine urea hydrochloride or other agent into sclerosed vessels, with resultant swelling and dying of the vessel, with reabsorption within the body.
- Banding the hemorrhoid may also be performed, this involves the application of a rubber band around the base of each hemorrhoid, which ultimately results in the death and necrosis of the hemorrhoid.
- Laser surgery may also be performed but symptomatic relief is not obtained immediately.
- Hemorrhoidectomy is performed if the patient has internal hemorrhoids with prolapse, or if the patient has both internal and external hemorrhoids. It relieves symptoms immediately but can create scar tissues and other complications; should be done as a last resort.
- Instruct patient and/or family regarding causes of hemorrhoids, methods of avoiding hemorrhoids, and treatments that can be performed.
- Rationale: Hemorrhoids are caused by straining, heavy lifting, obesity, pregnancy, and any activity that distends rectal veins and causes them to prolapse.
- Instruct patient and/or family regarding all procedures required.
- Rationale: Internal hemorrhoids are normally diagnosed by anoscopy or flexible sigmoidoscopy because digital rectal exam cannot adequately detect hemorrhoids. Barium enemas or colonoscopy may be required to ensure that intestinal masses are not presence as well.
- Instruct patient and/or family in dietary management.
- Rationale: Increasing bulk, fiber, fluids, and eating fruits and vegetables can help by maintaining soft stools to avoid straining at bowel movements.
- Instruct patient and/or family regarding the use of bulk producing agents, such as psyllium husk.
- Rationale: Bulk-forming laxatives help absorb water to increase moisture content in the stool, increases peristalsis, and helps promote soft bowel movements.
- Instruct patient and/or family in comfort measures to use with the presence of hemorrhoids.
- Rationale: Use of rubber donuts remove pressure directly placed on the hemorrhoid. Warm sitz baths or suppositories containing anesthetic agents can help to alleviate pain temporarily.
Nursing Diagnosis
Constipation
May be related to
- Low residue diet
- Lack of dietary bulk
- Hemorrhoidal pain
- Medications
Possibly evidenced by
- Passage of hard, formed stool
- Decreased bowel sounds
- Inability to evacuate stool
- Severe, exquisite rectal pain
- Abdominal pain
- Abdominal distention
- Ileus
- Absent bowel sounds
- Frequency of stool is less than normal
- Less than usual amount of stool
- Palpable mass
- Feeling of rectal fullness
- Flatulence
Desired Outcomes
- Patient will have normal elimination pattern reestablished and maintained.
Nursing Interventions
- Determine patient’s bowel habits, lifestyle, ability to sense urge to defecate, painful hemorrhoids, and history of constipation.
- Rationale: Assists with identification of an effective bowel regimen and/or impairment, and need for assistance. GI function may be decreased as a result of decreased digestion. Functional impairment related to muscular weakness and immobility may result in decreased abdominal peristalsis and difficulty with identification of the urge to defecate.
- Assess patient’s stool frequency, characteristics, presence of flatulence, abdominal discomfort or distension, and straining at stool.
- Rationale: Aging, such as decreased rectal compliance, pain, impairment of rectal sensation can lead to constipation.
- Auscultate bowel sounds of presence and quality.
- Rationale: Abnormal sounds, such as high-pitched tinkles, suggests complications like ileus.
- Monitor diet and fluid intake.
- Rationale: Adequate amounts of fiber and roughage provide bulk and adequate fluid intake of at least 2 L per day is important in keeping the stool soft.
- Monitor for complaints of abdominal pain and abdominal distention.
- Rationale: Gas, abdominal distention, or ileus, could be a factor. Lack of peristalsis from impaired digestion can create bowel distention and worse to the point of ileus.
- Monitor patient’s mental status, syncope, chest pain, or any transient ischemic attacks. Notify the physician if these symptoms occur.
- Rationale: Undue straining may have harmful effects on arterial circulation that can result in cardiac, cerebral, or peripheral ischemia.
- Assess for rectal bleeding.
- Rationale: Excessive straining may produce hemorrhoids, rectal prolapse, or anal fissures, with resultant pain and bleeding.
- Provide bulk, stool softeners, laxatives, suppositories, or enemas as warranted.
- Rationale: May be used to stimulation evacuation of stool.
- Provide high-fiber diet, whole grain cereals, breads, and fresh fruits.
- Rationale: Improves peristalsis and promotes elimination.
- Monitor medications that may predispose patient to constipation.
- Rationale: Analgesics, anesthetics, anticholinergics, diuretics, and other drugs are some medications that are known to cause constipation.
- Instruct patient in activity or exercise programs within limits of disease process.
- Rationale: Activity promotes peristalsis and stimulates defecation. Exercises help to strengthen the abdominal muscles that aid in defecation.
Nursing Diagnosis
Acute Pain
May be related to
- Hemorrhoidal pain
- GI bleeding
- Gastric mucosal irritation
- Inflammation
- Infection
- Constipation
- Spasm
- Surgery
Possibly evidenced by
- Verbalization of pain
- Fever
- Malaise
- Rectal pain
- Elevated WBC
- Surgical wounds
- Drains
- Tachycardia
- Hypertension
- Tachypnea
- Facial grimacing
- Crying
- Moaning
- Rectal bleeding
- Rectal pruritus
- Rectal burning
Desired Outcomes
- Patient will achieve relief from aches and pain
- Patient will report pain is controlled or eliminated
Nursing Interventions
- Assess patient for complaints of headaches, sore throat, general malaise or body weakness, muscle aches and pain.
- Rationale: Caused by inflammation or elevated temperature.
- Assess VS for changes from baselines
- Rationale: VS are usually increased as result of autonomic response to pain.
- Administer analgesics as ordered.
- Rationale: Pharmacologic therapy to control pain and aches by inhibiting brain prostaglandin synthesis.
- Provide restful, quiet environment.
- Rationale: Reduces stimuli that may increase pain.
- Provide warm baths or heating pad to aching muscles.
- Rationale: Warmth causes vasodilation and decreases discomfort.
- Provide cool compress to head prn.
- Rationale: Promotes comfort and treats headache.
- Provide backrubs prn.
- Rationale: Promotes relaxation and relieves aches.
- Encourage gargling with warm water; provide throat lozenges as necessary.
- Rationale: Reduces throat discomfort.
- Instruct patient or SO in deep breathing, relaxation techniques, guided imagery, massage and other nonpharmacologic aids.
- Rationale: Helps patient to focus less on pain, and may improve efficacy of analgesics by decreasing muscle tension.
- Instruct patient or SO regarding use of acetaminophen and to avoid use of aspirin.
- Rationale: Acetaminophen may relieve pain and headache, but should be used cautiously in patients with liver dysfunction because of acetaminophen metabolism in the liver. Aspirin can potentially cause hemorrhage and ulceration, therefore, must be avoided.

")