Notes
Description
There are two major forms of acute leukemia: lymphocytic leukemia and nonlymphocytic leukemia. Lymphocytic leukemia involves the lymphocytes (cells that are derived from the stem cells and circulate among the blood, lymph nodes, and lymphatic organs) and lymphoid organs; nonlymphocytic leukemia involves hematopoietic stem cells that differentiate into monocytes, granulocytes, red blood cells (RBCs), and platelets. Up to 90% of acute leukemias are a form of lymphocytic leukemia, acute lymphoblastic leukemia (ALL), which is characterized by the abnormal growth of lymphocyte precursors called lymphoblasts. Acute myelogenous leukemia (AML) (also known as acute nonlymphocytic leukemia, or ANLL) causes the rapid accumulation of megakaryocytes (precursors to platelets), monocytes, granulocytes, and RBCs. As the disease progresses, the patient may have central nervous system (CNS) dysfunction with seizures, decreased mental status, or coma and renal insufficiency. Death occurs when the abnormal cells encroach on vital tissues and cause complications and organ dysfunction.
Causes
- The exact cause of acute leukemia is unknown, but there are several risk factors. Overexposure to radiation even years before the development of the disease, particularly if the exposure is prolonged, is a major risk factor. Other risk factors include exposure to certain chemicals (benzene),medications (alkylating agents used to treat other cancers in particular), and viruses. Other related factors in children include genetic abnormalities such as Down syndrome, albinism, and congenital immunodeficiency syndrome. People who have been treated with chemotherapeutic agents for other forms of cancer have an increased risk for developing AML. Such cases generally develop within 9 years of chemotherapy.
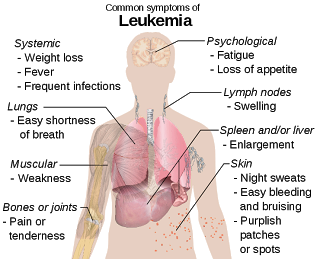
Signs and Symptoms
- The patient appears acutely ill, short of breath, and pale.
- Children are often febrile.
- When you inspect the lips and mouth, you may note bleeding gums and ulcerated areas of the mouth and throat.
- On palpation, you may feel lymph node swelling and enlargement of the liver and spleen.
- When you auscultate the patient’s lungs, you may hear decreased breath sounds, shallow and rapid respirations, a rapid heart rate, and a systolic ejectionmurmur.
Diagnostic Evaluation
- CBC and blood smear – peripheral WBC count varies widely from 1,000 to 100,000/mm3 and may include significant numbers of abnormal immature (blast) cells, anemia may be profound; platelet count may be abnormal and coagulopathies may exist.
- Bone marrow aspiration and biopsy – cells also studied for chromosomal abnormalities (cytogenetics) and immunologic markers to classify type of leukemia further.
- Lymph node biopsy – to detect the spread.
- Lumbar puncture and examination of cerebrospinal fluid for leukemic cells (especially ALL).
PRIMARY NURSING DIAGNOSIS
- Risk for infection related to decreased primary and secondary responses
- OUTCOMES. Immune status; Knowledge: Infection control; Risk control; Risk detection;Nutrition status; Treatment behavior: Illness or injury; Hydration; Knowledge: Infection control
- INTERVENTIONS. Infection control; Infection protection; Surveillance; Fluid/electrolyte management; Medication management; Temperature regulation
Pharmacologic Interventions
Different types of leukemia are best treated with different kinds of medicine.
- Acute lymphoblastic leukemia (ALL) drugs include prednisone, vincristine, daunorubicin, L-asparaginase or pegaspargase, methotrexate, and cyclophosphamide. Imatinib (Gleevec) is sometimes used to treat ALL. Dasatinib (Sprycel) is a newer drug for treating some ALL that has not improved with other drugs.
- Acute myelogenous leukemia (AML) drugs include daunorubicin, idarubicin, cytosine arabinoside, and mitoxantrone.10 Gemtuzumab (Mylotarg) may be given to people whose AML has relapsed. It helps your body destroy cancer cells.
- Acute promyelocytic leukemia (APL) drugs include all-trans-retinoic acid (ATRA) and chemotherapy with arsenic trioxide, idarubicin, or daunorubicin. ATRA helps control the risk of life-threatening bleeding from disseminated intravascular coagulation (DIC). Later treatment can include ATRA with or without methotrexate and 6-mercaptopurine. Or if a first round of ATRA and chemotherapy does not work, arsenic trioxide may be used.
- To treat leukemia in the brain or prevent it from spreading to the brain and central nervous system, methotrexate and cytarabine/cytosine arabinoside are injected into the spinal canal. This is called intrathecal chemotherapy.
Supportive treatments during cancer treatment include:
- Antibiotics and immunoglobulins help to prevent or fight infections. This is important when you do not have enough normal white blood cells to fight infections on your own.
- Transfusions of red blood cells and platelets.
- Epoetin and hematopoietic stimulants help your body make new blood cells.
- Allopurinol to prevent kidney problems and gout.
- Saline or steroid eyedrops for relief during treatment with cytarabine/cytosine arabinoside.
Medical Management
- The treatment for acute leukemia occurs in four phases: induction, consolidation, continuation, and treatment of (CNS) leukemia. During the induction phase, the patient receives an intense course of chemotherapy that is meant to cause a complete remission of the disease. Complete remission occurs when the patient has less than 5% of the bone marrow cells as blast cells and the peripheral blood counts are normal. Once remission has been sustained for 1 month, the patient enters the consolidation phase, during which she or he receives a modified course of chemotherapy to eradicate any remaining disease. The continuation, or maintenance, phase may continue for more than a year, during which time the patient receives small doses of chemotherapy every 3 to 4 weeks. Treatment of CNS leukemia is an essential component of therapy that has replaced irradiation, which leads to significant CNS complications, with intensive intrathecal and systemic chemotherapy for most patients.
- Some patients also need transfusions with blood component therapy to control infection and prevent bleeding and anemia. Bone marrow transplantation (BMT) is an option for some patients. Early BMTs were allogenic transplants using stem cells that had been harvested from bone marrow from siblings or matched from unrelated relatives. In autologous BMTs in the 1980s, physicians began using frozen cells harvested from the donor’s own marrow during remission. More recently, a newer form of transplant has occurred with peripheral blood stem cell transplant (SCT) or peripheral blood progenitor cell transplant. Multiple pheresis, or removal of cells from the blood, provides the stem cells from the patient for transplantation. SCT permits the use of doses of chemotherapy and radiation therapy high enough to destroy the patient’s bone marrow; after the treatment is completed SCT restores blood-producing bone marrow stem cells. Radiation treatment is sometimes used to treat leukemic cells in the brain, spinal cord, or testicles.
Nursing Interventions
Preventing infection:
- Frequently monitor the client for pneumonia, pharyngitis, esophagitis, perianal cellulitis, urinary tract infection, and cellulitis, which are common in leukemia and which carry significant morbidity and mortality.
- Monitor for fever, flushed appearance, chills, tachycardia; appearance of white patches in the mouth; redness, swelling, heat or pain in the eyes, ears, throat, skin, joints, abdomen, rectal and perineal areas; cough, changes in sputum; skin rash.
- Check results of granulocyte counts. Concentrations less than 500/mm3 put the patient at serious risk for infection.
- Avoid invasive procedures and trauma to skin or mucous membrane to prevent entry of microorganisms.
- Use the following rectal precautions to prevent infections: Avoid diarrhea and constipation, which can irritate the rectal mucosa, avoid the use of rectal thermometers, and keep perineal are clean.
- Care for the patient in private room with strict handwashing practice.
- Encourage and assist patient with personal hygiene, bathing, and oral care.
- Obtain cultures and administer antimicrobials promptly as directed.
Preventing and Managing bleeding:
- Watch for signs of minor bleeding, such as petechiae, ecchymosis, conjunctival hemorrhage, epistaxis, bleeding gums, bleeding at puncture sites, vaginal spotting, heavy menses.
- Be alert for signs of serious bleeding, such as headache with change in responsiveness, blurred vision, hemoptysis, hematemesis, melena, hypotension, tachycardia, dizziness.
- Test all urine, stool, emesis for gross and occult blood.
- Monitor platelet counts daily.
- Administer blood components as directed.
- Keep patient on bed rest during bleeding episodes.
Patient Education and Health Maintenance:
- Teach signs and symptoms of infection and advise whom to notify.
- Encourage adequate nutrition to prevent emaciation from chemotherapy.
- Teach avoidance of constipation with increased fluid and fiber, and good perineal care.
- Teach bleeding precautions.
- Encourage regular dental visits to detect and treat dental infections and disease.
- http://nursingcrib.com/case-study/leukemia-case-study/
- http://www.cancer.gov/dictionary?cdrid=45145
- http://www.cancer.org/cancer/leukemia-acutelymphocyticallinadults/detailedguide/leukemia-acute-lymphocytic-risk-factors
- Diseases and Disorders a Therapeutic Manual, 2007
Exam
Nursing Care Plan
Nursing Priorities
- Prevent infection during acute phases of disease/treatment.
- Maintain circulating blood volume.
- Alleviate pain.
- Promote optimal physical functioning.
- Provide psychological support.
- Provide information about disease process/prognosis and treatment needs.
Nursing diagnosis: Infection, risk for
Risk factors may include
- Inadequate secondary defenses: alterations in mature WBCs (low granulocyte and abnormal lymphocyte count), increased number of immature lymphocytes; immunosuppression, bone marrow suppression (effects of therapy/transplant)
- Inadequate primary defenses (stasis of body fluids, traumatized tissue)
- Invasive procedures
- Malnutrition; chronic disease
Possibly evidenced by
Not applicable; presence of signs and symptoms establishes an actual diagnosis.
Desired outcomes/evaluation criteria—patient will:
Knowledge: Infection Control (NOC)
- Identify actions to prevent/reduce risk of infection.
Demonstrate techniques, lifestyle changes to promote safe environment, achieve timely healing.
Nursing Interventions
Infection Protection
Independent
- Place in private room. Screen/limit visitors as indicated. Prohibit use of live plants/cut flowers. Restrict fresh fruits and vegetables or make sure they are washed or peeled.
- Rationale: Protect patient from potential sources of pathogens/infection. Note: Profound bone marrow suppression, neutropenia, and chemotherapy place patient at great risk for infection.
- Require good handwashing protocol for all personnel and visitors.
- Rationale: Prevents cross-contamination/reduces risk of infection.
- Monitor temperature. Note correlation between temperature elevations and chemotherapy treatments. Observe for fever associated with tachycardia, hypotension, subtle mental changes.
- Rationale: Although fever may accompany some forms of chemotherapy, progressive hyperthermia occurs in some types of infections, and fever (unrelated to drugs or blood products) occurs in most leukemia patients. Note: Septicemia may occur without fever.
- Prevent chilling. Force fluids, administer tepid sponge bath.
- Rationale: Helps reduce fever, which contributes to fluid imbalance, discomfort, and CNS complications.
- Encourage frequent turning and deep breathing.
- Rationale: Prevents stasis of respiratory secretions, reducing risk of atelectasis/pneumonia.
- Auscultate breath sounds, noting crackles, rhonchi; inspect secretions for changes in characteristics, e.g., increased sputum production or change in sputum color. Observe urine for signs of infection, e.g. cloudy, foul-smelling, or presence of urgency or burning with voids.
- Rationale: Early intervention is essential to prevent sepsis/septicemia in immunosuppressed person.
- Handle patient gently. Keep linens dry/wrinkle-free.
- Rationale: Prevents sheet burn/skin excoriation.
- Inspect skin for tender, erythematous areas; open wounds. Cleanse skin with antibacterial solutions.
- Rationale: May indicate local infection. Note: Open wounds may not produce pus because of insufficient number of granulocytes.
- Inspect oral mucous membranes. Provide good oral hygiene. Use a soft toothbrush, sponge, or swabs for frequent mouth care.
- Rationale: The oral cavity is an excellent medium for growth of organisms and is susceptible to ulceration and bleeding.
- Promote good perianal hygiene. Examine perianal area at least daily during acute illness. Provide sitz baths, using Betadine or Hibiclens if indicated. Avoid rectal temperatures, use of suppositories.
- Rationale: Promotes cleanliness, reducing risk of perianal abscess; enhances circulation and healing. Note: Perianal abscess can contribute to septicemia and death in immunosupressed patients.
- Coordinate procedures and tests to allow for uninterrupted rest periods.
- Rationale: Conserves energy for healing, cellular regeneration.
- Encourage increased intake of foods high in protein and fluids with adequate fiber.
- Rationale: Promotes healing and prevents dehydration. Note: Constipation potentiates retention of toxins and risk of rectalirritation/tissue injury.
- Avoid/limit invasive procedures (e.g. venipuncture and injections) as possible.
- Rationale: Break in skin could provide an entry for pathogenic/potentially lethal organisms. Use of central venous lines (e.g., tunneled catheter or implanted port) can effectively reduce need for frequent invasive procedures and risk of infection. Note:Myelosuppression may be cumulative in nature, especially when multiple drug therapy (including steroids) is prescribed.
Collaborative
- Monitor laboratory studies, e.g.: CBC, noting whether WBC count falls or sudden changes occur in neutrophils;
- Decreased numbers of normal/mature WBCs can result from the disease process or chemotherapy, compromising the immune response and increasing risk of infection.
- Gram’s stain cultures/sensitivity.
- Rationale: Verifies presence of infections; identifies specific organisms and appropriate therapy.
- Review serial chest x-rays.
- Rationale: Indicator of development/resolution of respiratory complications.
- Prepare for/assist with leukemia-specific treatments such as chemotherapy, radiation, and/or bone marrow transplant.
- Rationale: Leukemia is usually treated with a combination of these agents, each requiring specific safety precautions for patient and care providers.
- Administer medications as indicated, e.g.: antibiotics;
- Rationale: May be given prophylactically or to treat specific infection.
- Colony-stimulating factors: sargramostim (Leukine).
- Rationale: Restores WBCs destroyed by chemotherapy and reduces risk of severe infection and death in certain types of leukemia.
- Avoid use of aspirin-containing antipyretics.
- Rationale: Aspirin can cause gastric bleeding and further decrease platelet count.
- Provide nutritious diet, high in protein and calories, avoiding raw fruits, vegetables, or uncooked meats.
- Rationale: Proper nutrition enhances immune system. Minimizes potential sources of bacterial contamination.
Nursing diagnosis: Fluid Volume, risk for deficient
Risk factors may include
- Excessive losses, e.g., vomiting, hemorrhage, diarrhea
- Decreased fluid intake, e.g., nausea, anorexia
- Increased fluid need, e.g., hypermetabolic state, fever; predisposition for kidney stone formation/tumor lysis syndrome
Possibly evidenced by
Not applicable; presence of signs and symptoms establishes an actual diagnosis.
Desired outcomes/evaluation criteria—patient will:
- Demonstrate adequate fluid volume, as evidenced by stable vital signs; palpable pulses; urine output, specific gravity, and pH within normal limits.
- Identify individual risk factors and appropriate interventions.
- Initiate behaviors/lifestyle changes to prevent development of dehydration.
Nursing Intervention
Fluid Management
Independent
- Monitor I&O. Calculate insensible losses and fluid balance. Note decreased urine output in presence of adequate intake. Measure specific gravity and urine pH.
- Rationale: Tumor lysis syndrome occurs when destroyed cancer cells release toxic levels of potassium, phosphorus, and uric acid. Elevated phosphorus and uric acid levels can cause crystal formation in the renal tubules, impairing filtration and leading to renal failure.
- Weigh daily.
- Rationale: Measure of adequacy of fluid replacement and kidney function. Continued intake greater than output may indicate renal insult/obstruction.
- Monitor BP and HR.
- Rationale: Changes may reflect effects of hypovolemia (bleeding/dehydration).
- Evaluate skin turgor, capillary refill, and general condition of mucous membranes.
- Rationale: Indirect indicators of fluid status/hydration.
- Note presence of nausea, fever.
- Rationale: Affects intake, fluid needs, and route of replacement.
- Encourage fluids of up to 3–4 L/day when oral intake is resumed.
- Rationale: Promotes urine flow, prevents uric acid precipitation, and enhances clearance of antineoplastic drugs.
Bleeding Precautions
Independent
- Inspect skin/mucous membranes for petechiae, ecchymotic areas; note bleeding gums, frank or occult blood in stools and urine; oozing from invasive-line sites.
- Rationale: Suppression of bone marrow and platelet production places patient at risk for spontaneous/uncontrolled bleeding.
- Implement measures to prevent tissue injury/bleeding, e.g., gentle brushing of teeth or gums with soft toothbrush, cotton swab, or sponge-tipped applicator; using electric razor and avoiding sharp razors when shaving; avoiding forceful nose blowing and needlesticks when possible; using sustained pressure (sandbags or pressure dressings) on oozing puncture/IV sites.
- Rationale: Fragile tissues and altered clotting mechanisms increase the risk of hemorrhage following even minor trauma.
- Limit oral care to mouthwash if indicated (a mixture of 1/4 tsp baking soda or salt in 4–8 oz water or hydrogen peroxide in water). Avoid mouthwashes with alcohol.
- Rationale: When bleeding is present, even gentle brushing may cause more tissue damage. Alcohol has a drying effect and may be painful to irritated tissues.
- Provide soft diet.
- Rationale: May help reduce gum irritation.
Fluid Management
Collaborative
- Administer IV fluids as indicated.
- Rationale: Maintains fluid/electrolyte balance in the absence of oral intake; prevents or minimizes tumor lysis syndrome, reduces risk of renal complications.
- Administer medications as indicated, e.g.Antiemetics: 5-HT3 receptor antagonist drugs such as ondansetron (Zofran) or granisetron (Kytril)
- Rationale: Relieves nausea/vomiting associated with administration of chemotherapy agents.
- Allopurinol (Zyloprim)
- Rationale: Improves renal excretion of toxic byproducts from breakdown of leukemia cells. Reduces the chances of nephropathy as a result of uric acid production.
- Potassium acetate or citrate, sodium bicarbonate
- Rationale: May be used to alkalinize the urine, preventing or minimizing tumor lysis syndrome/kidney stones.
- Stool softeners.
- Rationale: Helpful in reducing straining at stool with trauma to rectal tissues.
Bleeding Precautions
- Monitor laboratory studies, e.g. platelets, Hb/Hct, clotting.
- Rationale: When the platelet count is less than 20,000/mm (because of proliferation of WBCs and/or bone marrow suppression secondary to antineoplastic drugs), patient is prone to spontaneous life-threatening bleeding. Decreasing Hb/Hct is indicative of bleeding (may be occult).
Collaborative
- Administer RBCs, platelets, clotting factors.
- Rationale: Restores/normalizes RBC count and oxygen-carrying capacity to correct anemia. Used to prevent/treat hemorrhage.
- Maintain external central vascular access device (subclavian or tunneled catheter or implanted port).
- Rationale: Eliminate peripheral venipuncture as source of bleeding.
- Administer medications, e.g. oral contraceptives
- Rationale: Minimizes blood loss by stopping or slowing menstrual flow.
Nursing diagnosis: Pain, acute
May be related to
- Physical agents, e.g. enlarged organs/lymph nodes, bone marrow packed with leukemic cells
- Chemical agents, e.g. antileukemic treatments
- Psychological manifestations, e.g. anxiety, fear
Possibly evidenced by
- Reports of pain (bone, nerve, headaches, and so forth)
- Guarding/distraction behaviors, facial grimacing, alteration in muscle tone
- Autonomic responses
Desired outcomes/evaluation criteria—patient will:
Pain Level (NOC)
- Report pain is relieved/controlled.
- Appear relaxed and able to sleep/rest appropriately.
Pain Control (NOC)
- Demonstrate behaviors to manage pain.
Nursing Intervention
Pain Management
Independent
- Investigate reports of pain. Note changes in degree (use scale of 0–10) and site.
- Rationale: Helpful in assessing need for intervention; may indicate developing complications.
- Monitor vital signs, note nonverbal cues, e.g. muscle tension, restlessness.
- Rationale: May be useful in evaluating verbal comments and effectiveness of interventions.
- Provide quiet environment and reduce stressful stimuli, e.g. noise, lighting, constant interruptions.
- Rationale: Promotes rest and enhances coping abilities.
- Place in position of comfort and support joints, extremities with pillows/padding.
- Rationale: May decrease associated bone/joint discomfort.
- Reposition periodically and provide/assist with gentle ROM exercises.
- Rationale: Improves tissue circulation and joint mobility.
- Provide comfort measures (e.g. massage, cool packs) and psychological support (e.g. encouragement, presence).
- Rationale: Minimizes need for/enhances effects of medication.
- Review/promote patient’s own comfort interventions, e.g. position, physical activity/nonactivity, and so forth.
- Rationale: Successful management of pain requires patient involvement. Use of effective techniques provides positive reinforcement, promotes sense of control, and prepares patient for interventions to be used after discharge.
- Evaluate and support patient’s coping mechanisms.
- Rationale: Using own learned perceptions/behaviors to manage pain can help patient cope more effectively.
- Encourage use of stress management techniques, e.g. relaxation/deep-breathing exercises, guided imagery, visualization; Therapeutic Touch.
- Rationale: Facilitates relaxation, augments pharmacological therapy, and enhances coping abilities.
- Assist with/provide diversional activities, relaxation techniques.
- Rationale: Helps with pain management by redirecting attention.
Collaborative
- Monitor uric acid level as appropriate.
- Rationale: Rapid turnover and destruction of leukemic cells during chemotherapy can elevate uric acid, causing swollen painful joints in some patients. Note: Massive infiltration of WBCs into joints can also result in intense pain.
- Administer medications as indicated:Analgesics, e.g. acetaminophen (Tylenol)
- Rationale: Given for mild pain not relieved by comfort measures.Note: Avoid aspirin-containing products because they may potentiate hemorrhage.
- Opioids, e.g., codeine, morphine, hydromorphone (Dilaudid);
- Rationale: Used around-the-clock, rather than prn, when pain is severe. Note: Use of patient-controlled analgesia (PCA) is beneficial in preventing peaks and valleys associated with intermittent drug administration and increases patient’s sense of control.
- Antianxiety agents, e.g., diazepam (Valium), lorazepam (Ativan).
- Rationale: May be given to enhance the action of analgesics/opioids.
Nursing diagnosis: Activity intolerance
May be related to
- Generalized weakness; reduced energy stores, increased metabolic rate from massive production of leukocytes
- Imbalance between oxygen supply and demand (anemia/hypoxia)
- Therapeutic restrictions (isolation/bedrest); effect of drug therapy
Possibly evidenced by
- Verbal report of fatigue or weakness
- Exertional discomfort or dyspnea
- Abnormal HR or BP response
Desired outcomes/evaluation criteria—patient will:
Endurance (NOC)
- Report a measurable increase in activity tolerance.
- Participate in ADLs to level of ability.
- Demonstrate a decrease in physiological signs of intolerance; e.g. pulse, respiration, and BP remain within patient’s normal range.
Nursing Intervention
Energy Management
Independent
- Evaluate reports of fatigue, noting inability to participate in activities or ADLs.
- Rationale: Effects of leukemia, anemia, and chemotherapy may be cumulative (especially during acute and active treatment phase), necessitating assistance.
- Encourage patient to keep a diary of daily routines and energy levels, noting activities that increase fatigue.
- Rationale: Helps patient prioritize activities and arrange them around fatigue pattern.
- Provide quiet environment and uninterrupted rest periods. Encourage rest periods before meals.
- Rationale: Restores energy needed for activity and cellular regeneration/tissue healing.
- Implement energy-saving techniques, e.g., sitting, rather than standing, use of shower chair. Assist with ambulation/other activities as indicated.
- Rationale: Maximizes available energy for self-care tasks.
- Schedule meals around chemotherapy. Give oral hygiene before meals and administer antimetics as indicated.
- Rationale: May enhance intake by reducing nausea.
- Recommend small, nutritious, high-protein meals and snacks throughout the day.
- Rationale: Smaller meals require less energy for digestion than larger meals. Increased intake provides fuel for energy.
Collaborative
- Provide supplemental oxygen.
- Rationale: Maximizes oxygen available for cellular uptake, improving tolerance of activity.
Nursing diagnosis: Knowledge, deficient [Learning Need] regarding disease, prognosis, treatment, self-care, and discharge needs
May be related to
- Lack of exposure to resources
- Information misinterpretation/lack of recall
Possibly evidenced by
- Verbalization of problem/request for information
- Statement of misconception
Desired outcomes/evaluation criteria—patient will:
Knowledge: Illness Care (NOC)
- Verbalize understanding of condition/disease process and potential complications.
- Verbalize understanding of therapeutic needs.
- Initiate necessary lifestyle changes.
- Participate in treatment regimen.
Nursing Intervention
Teaching: Disease Process (NIC)
Independent
- Review pathology of specific form of leukemia and various treatment options.
- Rationale: Treatments can include various antineoplastic drugs, transfusions, peripheral progenitor (stem) cell transplant or bone marrow transplant.
References
- Canobbio, M. (2006). Mosby’s handbook of patient teaching. Elsevier Health Sciences
- Markman, M., Loguidice, C. & Lammersfeld, C. (2013). Cancer nutrition and recipes for dummies. Hoboken, NJ: John Wiley & Sons.


