Definition
- Peptic ulcer disease involves ulcers, circumscribed breaks in the mucosa, involving the duodenum (duodenal ulcers), the stomach (gastric ulcers) and less commonly the distal esophagus and the jejunum.
Risk Factors
- Peak incidence of duodenal ulcers (between ages 25 and 50); gastric ulcers (older than age 50)
- Helicobacter pylori infection
- altered gastric acid and serum gastrin levels
- tobacco smoking and alcohol use
- use of aspirin, other nonsteroidal anti-inflammatory drugs, and steroids
- genetic predisposition
- psychosomatic or psychological factors (e.g. chronic anxiety, type A personality)
Pathophysiology
- Normally, tightly packed epithelial cells protect the gastric mucosa from irritation. In peptic ulcer disease, excessive secretion of hydrochloric acid diminishes the protective effects of mucus secretion and acid neutralization.
- Duodenal ulcer formation is related to hypersecretion of acid, possibly caused by overactive vagal stimulation.
- Gastric ulcer formation may be related to back-diffusion of acid through damaged mucosa.
- Possible complications of peptic ulcer disease include perforation, hemorrhage, and pyloric obstruction.
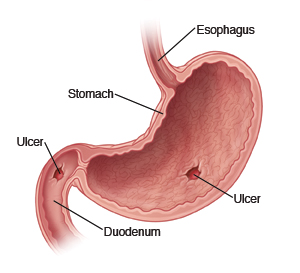
image by : http://www.uofmmedicalcenter.org/
Assessment/Clinical Manifestations/Signs and Symptoms
Duodenal ulcers
- Burning, aching, or gnawing pain in the right epigastrium occurring 2 to 3 hours after meals, possibly causing the client to awaken at night; relieved by eating
- Pyrosis (i.e. heartburn), nausea, and vomiting
- GI bleding, a slow oozing manifested by melena or a sudden, rapid loss of large amounts of blood through hematemesis.
- Epigastric tenderness
Gastric ulcers
- Burning, aching, gnawing pain in the upper epigastrium occurring 30 minutes to 1 hour after meals (rarely at night); unrelieved by eating
- Epigastric tenderness
Laboratory and diagnostic study findings:
- Barium swallow shows an ulcerated area.
- Endoscopy identifies inflammation of gastric mucosa, ulcers, and lesions; biopsy can determine the presence of H. pylori.
Medical Management
Possible procedures include: (Vagotomy, Pyloroplasty,Distal subtotal gastrectomy)
- Billroth I – gastrodudenostomy
- Billroth II – gastrojejunostomy
Nursing Management
Administer prescribed medications.
- Medications may include antacids, anticholinergics, histamine-receptor antagonist, proton-pump inhibitors, and mucosal protective agents.
- Medication for ulcers caused by H. pylori include bismuth subsalicylate, metronidazole, and tetracycline. These medications administered together eradiate H. pylori bacteria in the gastric mucosa.
Provide client and family teaching.
- Instruct the client to quit smoking, which decreases the secretion of bicarbonate from the pancreas into the duodenum, resulting in increased acidity in the duodenum.
- Teach the client about necessary lifestyle modifications aimed at decreasing stress and maximizing effective coping. Biofeedback, hypnosis, or behavior modification may be suggested.
Teach the client methods to minimize symptoms while maintaining adequate nutrition.
- Avoid foods that previously have caused pain. Specific dietary restrictions vary from client to client.
- Eat three regular meals a day, small, frequent meals are unnecessary as long as the medication is taken before meals.
- Avoid a diet rich in milk and creams, which are acid stimulants.
Prepare the client for diagnostic procedures, and provide postprocedure care.
- Prepare for barium swallow includes no oral intake after midnight and possible laxatives to clean the GI tract.
- After a barium swallow, administer a laxative if indicated to preventconstipation.
- Stools are monitored until all barium has been eliminated.
For the client undergoing gastroscopy.
- obtain informed consent, and instruct the client not to eat noir drink anything for 8 hours before the procedure.
- After the procedure, assess the gag reflex before the client consumes foods and fluids.
- Monitor for signs of perforation (e.g pain, bleeding, abdominal distention)
Prepare the client for surgery if indicated. (e.g. ulcers that have not responded to treatment after 12 to 16 weeks, life-threatening hemorrhage or perforation)
Preoperative care
- Obtain informed consent
- Clear and empty the GI tract by administering enemas and allowing nothing by mouth
Postoperative care
- Ensure that the nasogastric tube (surgically placed) is not manipulated
- Observe nasogastric tube aspirate
- Assess the surgical dressing
- Provide routine postoperative care
- Provide discharge teaching

 Analysis")
